

Laparoscopic versus conventional appendectomy--a meta-analysis of randomized controlled trials
- PMID: 21047410
- PMCID: PMC2988072
- DOI: 10.1186/1471-230X-10-129
Laparoscopic versus conventional appendectomy--a meta-analysis of randomized controlled trials
Abstract
Background: Although laparoscopic surgery has been available for a long time and laparoscopic cholecystectomy has been performed universally, it is still not clear whether open appendectomy (OA) or laparoscopic appendectomy (LA) is the most appropriate surgical approach to acute appendicitis. The purpose of this work is to compare the therapeutic effects and safety of laparoscopic and conventional "open" appendectomy by means of a meta-analysis.
Methods: A meta-analysis was performed of all randomized controlled trials published in English that compared LA and OA in adults and children between 1990 and 2009. Calculations were made of the effect sizes of: operating time, postoperative length of hospital stay, postoperative pain, return to normal activity, resumption of diet, complications rates, and conversion to open surgery. The effect sizes were then pooled by a fixed or random-effects model.
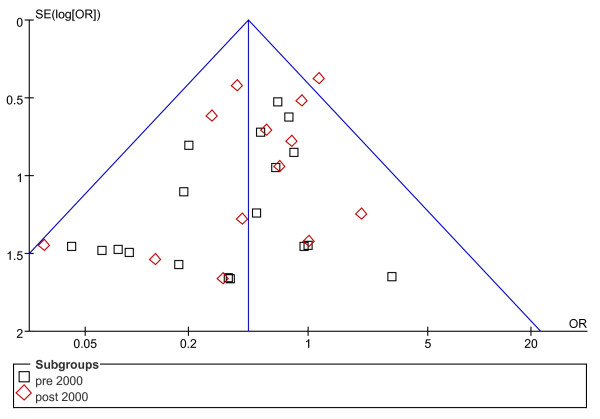
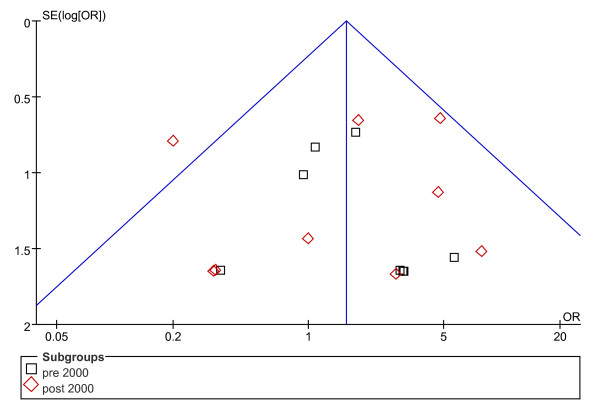
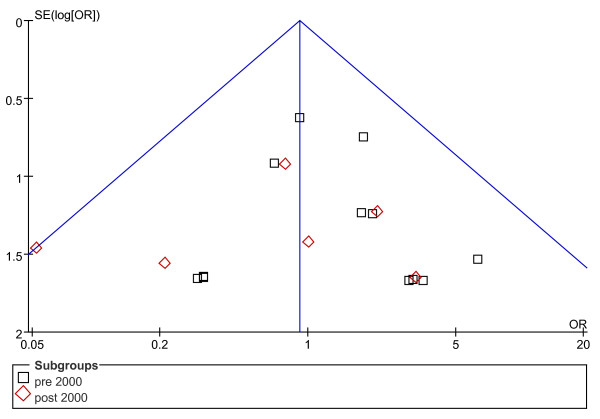
Results: Forty-four randomized controlled trials with 5292 patients were included in the meta-analysis. Operating time was 12.35 min longer for LA (95% CI: 7.99 to 16.72, p < 0.00001). Hospital stay after LA was 0.60 days shorter (95% CI: -0.85 to -0.36, p < 0.00001). Patients returned to their normal activity 4.52 days earlier after LA (95% CI: -5.95 to -3.10, p < 0.00001), and resumed their diet 0.34 days earlier(95% CI: -0.46 to -0.21, p < 0.00001). Pain after LA on the first postoperative day was significantly less (p = 0.008). The overall conversion rate from LA to OA was 9.51%. With regard to the rate of complications, wound infection after LA was definitely reduced (OR = 0.45, 95% CI: 0.34 to 0.59, p < 0.00001), while postoperative ileus was not significantly reduced(OR = 0.91, 95% CI: 0.57 to 1.47, p = 0.71). However, intra-abdominal abscess (IAA), intraoperative bleeding and urinary tract infection (UIT) after LA, occurred slightly more frequently(OR = 1.56, 95% CI: 1.01 to 2.43, p = 0.05; OR = 1.56, 95% CI: 0.54 to 4.48, p = 0.41; OR = 1.76, 95% CI: 0.58 to 5.29, p = 0.32).
Conclusion: LA provides considerable benefits over OA, including a shorter length of hospital stay, less postoperative pain, earlier postoperative recovery, and a lower complication rate. Furthermore, over the study period it was obvious that there had been a trend toward fewer differences in operating time for the two procedures. Although LA was associated with a slight increase in the incidence of IAA, intraoperative bleeding and UIT, it is a safe procedure. It may be that the widespread use of LA is due to its better therapeutic effect.
Figures

References
-
- Addiss DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990;132:910–925. (PMID: 2239906) - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
