

Review
doi: 10.1590/s1807-59322010000900014.
Difficult-to-control asthma management through the use of a specific protocol
Affiliations
- PMID: 21049219
- PMCID: PMC2954742
- DOI: 10.1590/s1807-59322010000900014
Item in Clipboard
Review
Difficult-to-control asthma management through the use of a specific protocol
Clinics (Sao Paulo).
2010.
Abstract
The present study is a critical review of difficult-to-control asthma, highlighting the characteristics and severity of the disease. It also presents a protocol for the management of patients with this asthma phenotype. The protocol, which was based on relevant studies in the literature, is described and analyzed.
Figures
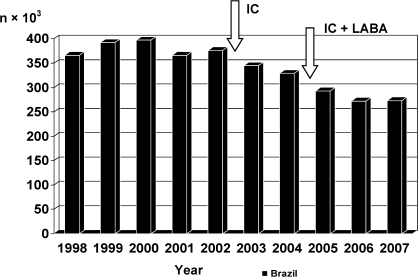
Hospitalization due to asthma in Brazil as a whole and in São Paulo, Brazil in particular, according to data from the Information Technology Department of the Brazilian Unified Health Care System.‐ Hospitalization due to asthma in Brazil as a whole and in São Paulo, Brazil in particular, according to data from the Information Technology Department of the Brazilian Unified Health Care System. IC: inhaled corticosteroid; LABA: long‐acting β2 agonist
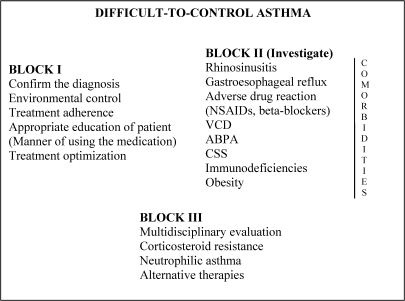
Protocol for the treatment of patients with difficult‐to‐control asthma.‐ Protocol for the treatment of patients with difficult‐to‐control asthma. VCD: vocal cord dysfunction; ABPA: allergic bronchopulmonary aspergillosis; NSAIDs: nonsteroidal anti‐inflammatory drugs; CSS: Churg‐Strauss syndrome
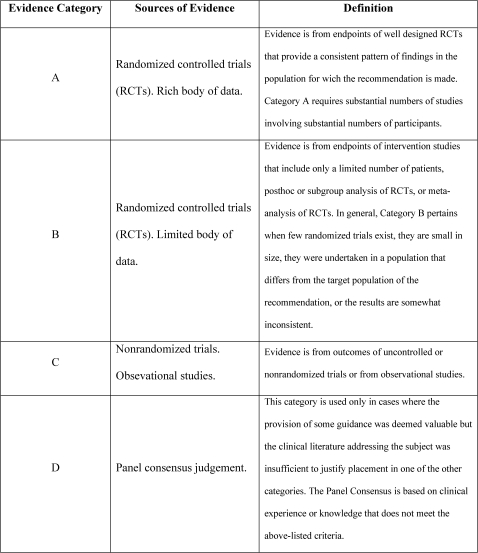
Description of levels of evidence (Adapted from GINA).‐ Description of levels of evidence (Adapted from GINA).
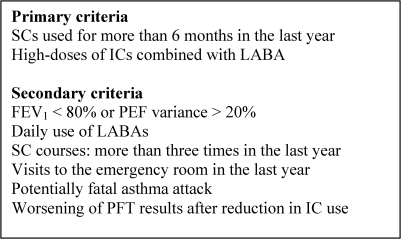
Criteria for the diagnosis of difficult‐to‐control asthma.‐ Criteria for the diagnosis of difficult‐to‐control asthma. SC: systemic corticosteroid; IC: inhaled corticosteroid; LABA: long‐acting β2 agonist; FEV1: forced expiratory volume in one second; PEF: peak expiratory flow; PFT: pulmonary function test
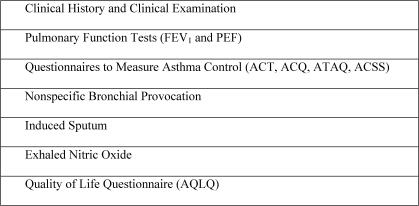
Assessment of asthma control.‐ Assessment of asthma control. FEV1: forced expiratory volume in one second; PEF: peak expiratory flow; ACT: asthma control test; ACQ: asthma control questionnaire; ATAQ: asthma therapy assessment questionnaire; ACSS: asthma control scoring system; AQLQ: asthma quality of life questionnaire
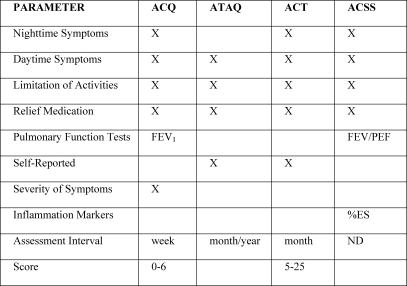
Questionnaires to measure asthma control.‐ Questionnaires to measure asthma control. ACT: asthma control test; ACQ: asthma control questionnaire; ATAQ: asthma therapy assessment questionnaire; ACSS: asthma control scoring system; FEV1: forced expiratory volume in one second; PEF: peak expiratory flow; and %ES: percentage of eosinophils in sputum; ND: not determined
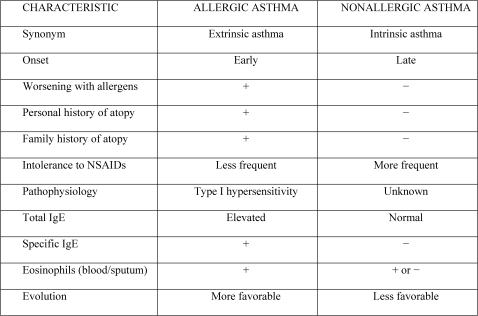
Differences between allergic asthma and non‐allergic asthma.‐ Differences between allergic asthma and non‐allergic asthma. NSAID: nonsteroidal anti‐inflammatory drug; IgE: immunoglobulin E
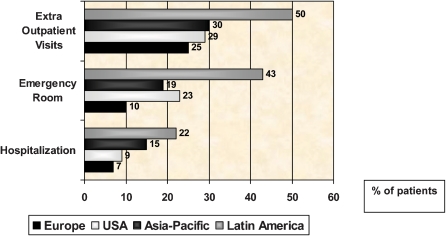
Rate of severe exacerbations of asthma in the last year.‐ Rate of severe exacerbations of asthma in the last year.
Objectives of the Allergic Rhinitis and its Impact on Asthma initiative.‐ Objectives of the Allergic Rhinitis and its Impact on Asthma initiative.
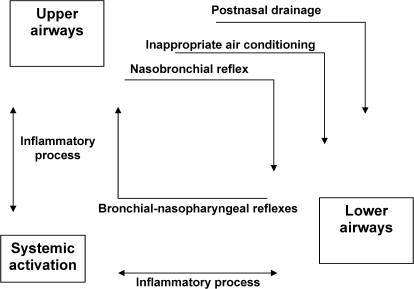
Pathophysiological evidence for the interaction between allergic rhinitis and allergic asthma.‐ Pathophysiological evidence for the interaction between allergic rhinitis and allergic asthma.
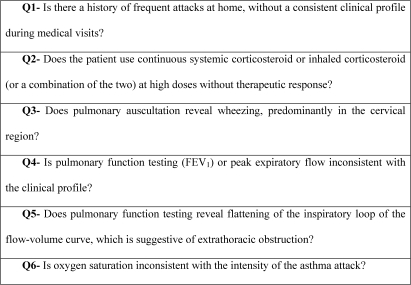
Specific questionnaire for the clinical suspicion of vocal cord dysfunction.‐ Specific questionnaire for the clinical suspicion of vocal cord dysfunction. Q: question;FEV1: forced expiratory volume in one second; and PEF: peak expiratory flow
References
-
- GINA. The Global Initiative for Asthma. Disponível em: www.ginasthma.com.
-
- Moorman JE, Rudd RA, Johnson CA, King M, Minor P, Bailey C, et al. National surveillance for asthma – United States, 1980‐2004. MMWR Surveill Summ. 2007;56:1–54. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
