

Phase II study of cilengitide (EMD 121974, NSC 707544) in patients with non-metastatic castration resistant prostate cancer, NCI-6735. A study by the DOD/PCF prostate cancer clinical trials consortium
- PMID: 21049281
- PMCID: PMC3175265
- DOI: 10.1007/s10637-010-9573-5
Phase II study of cilengitide (EMD 121974, NSC 707544) in patients with non-metastatic castration resistant prostate cancer, NCI-6735. A study by the DOD/PCF prostate cancer clinical trials consortium
Abstract
Background: Integrins mediate invasion and angiogenesis in prostate cancer bone metastases. We conducted a phase II study of cilengitide, a selective antagonist of α(v)β(3) and α(v)β(5) integrins, in non-metastatic castration resistant prostate cancer with rising PSA.
Methods: Patients were observed for 4 weeks with PSA monitoring, and then treated with 2,000 mg IV of cilengitide twice weekly until toxicity/progression. PSA, circulating tumor cells (CTCs) and circulating endothelial cells (CECs) were monitored each cycle with imaging performed every three cycles. Primary end point was PSA decline by ≥ 50%. Secondary endpoints were safety, PSA slope, time to progression (TTP), overall survival (OS), CTCs, CECs and gene expression.
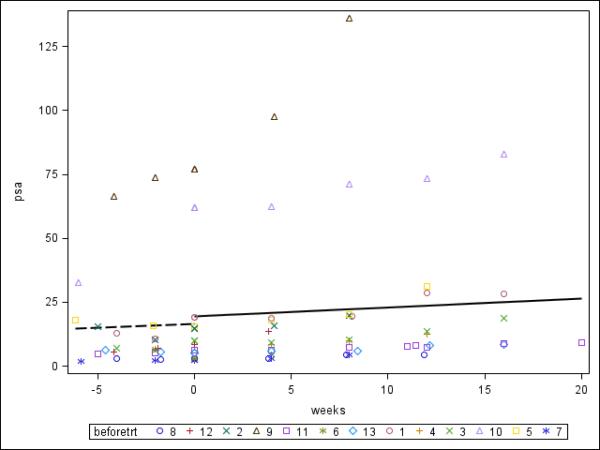
Results: 16 pts were enrolled; 13 were eligible with median age 65.5 years, baseline PSA 8.4 ng/mL and median Gleason sum 7. Median of three cycles was administered. Treatment was well tolerated with two grade three toxicities and no grade four toxicities. There were no PSA responses; 11 patients progressed by PSA after three cycles. Median TTP was 1.8 months and median OS has not been reached. Median pre- and on-treatment PSA slopes were 1.1 and 1.8 ng/mL/month. Baseline CTCs were detected in 1/9 patients. CTC increased (0 to 1; 2 pts), remained at 0 (2 pts) or decreased (23 to 0; 1 patient) at progression. Baseline median CEC was 26 (0-61) and at progression, 47 (15-148). Low cell counts precluded gene expression studies.
Conclusions: Cilengitide was well tolerated but had no detectable clinical activity. CTCs are of questionable utility in non-metastatic prostate cancer.
Figures


References
-
- Smith MR, Kabbinavar F, Saad F, Hussain A, Gittelman MC, Bilhartz DL, Wynne C, Murray R, Zinner NR, Schulman C, Linnartz R, Zheng M, Goessl C, Hei YJ, Small EJ, Cook R, Higano CS. Natural history of rising serum prostate-specific antigen in men with castrate nonmetastatic prostate cancer. J Clin Oncol. 2005;23(13):2918–2925. doi:23/13/2918 [pii] 10.1200/JCO.2005.01.529. - PubMed
-
- Ibrahim T, Flamini E, Mercatali L, Sacanna E, Serra P, Amadori D. Pathogenesis of osteoblastic bone metastases from prostate cancer. Cancer. 2010;116(6):1406–1418. doi:10.1002/cncr.24896. - PubMed
-
- Loberg RD, Logothetis CJ, Keller ET, Pienta KJ. Pathogenesis and treatment of prostate cancer bone metastases: Targeting the lethal phenotype. J Clin Oncol. 2005;23(32):8232–8241. doi:23/32/8232 [pii] 10.1200/JCO.2005.03.0841. - PubMed
-
- Felding-Habermann B. Integrin adhesion receptors in tumor metastasis. Clin Exp Metastasis. 2003;20(3):203–213. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
