

HIV-1 viral escape in cerebrospinal fluid of subjects on suppressive antiretroviral treatment
- PMID: 21050119
- PMCID: PMC3052942
- DOI: 10.1086/657342
HIV-1 viral escape in cerebrospinal fluid of subjects on suppressive antiretroviral treatment
Abstract
Background: Occasional cases of viral escape in cerebrospinal fluid (CSF) despite suppression of plasma human immunodeficiency virus type 1 (HIV-1) RNA have been reported. We investigated CSF viral escape in subjects treated with commonly used antiretroviral therapy regimens in relation to intrathecal immune activation and central nervous system penetration effectiveness (CPE) rank.
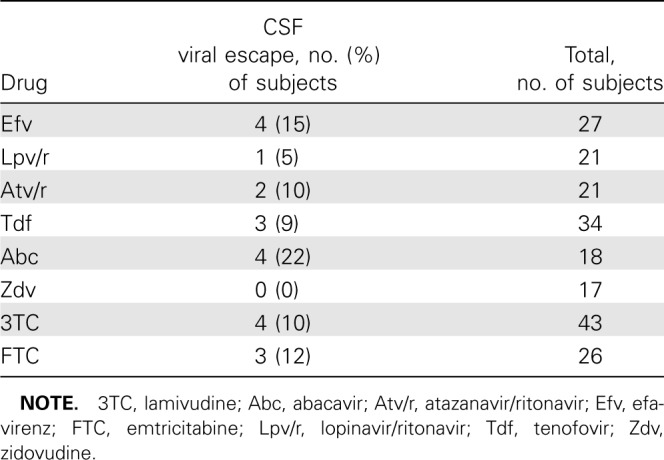
Methods: Sixty-nine neurologically asymptomatic subjects treated with antiretroviral therapy >6 months and plasma HIV-1 RNA <50 copies/mL were cross-sectionally included in the analysis. Antiretroviral therapy regimens included efavirenz, lopinavir/ritonavir or atazanavir/ritonavir combined with tenofovir, abacavir, or zidovudine and emtricitabine or lamivudine. HIV-1 RNA was analyzed with real-time polymerase chain reaction assays. Neopterin was analyzed by enzyme-linked immunosorbent assay.
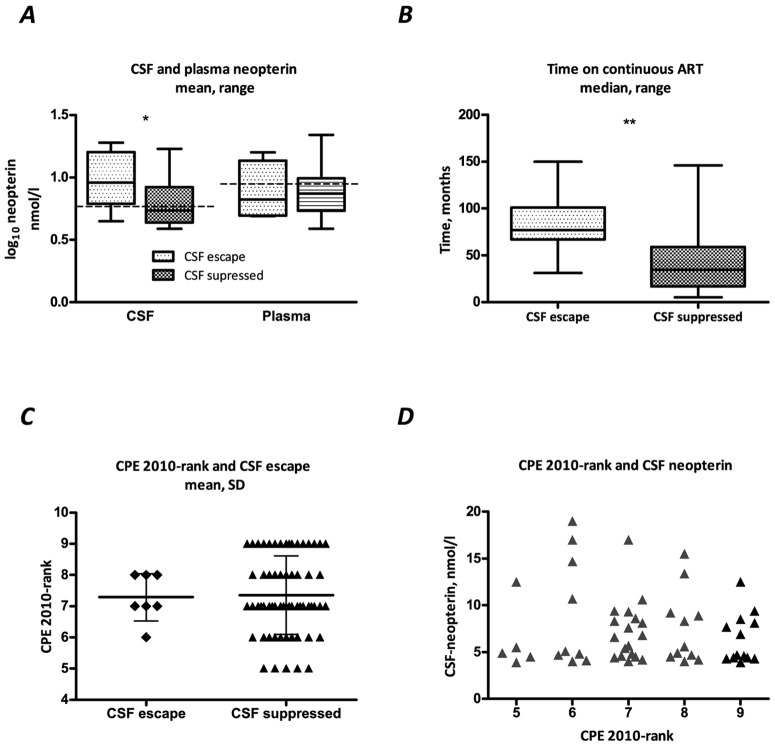
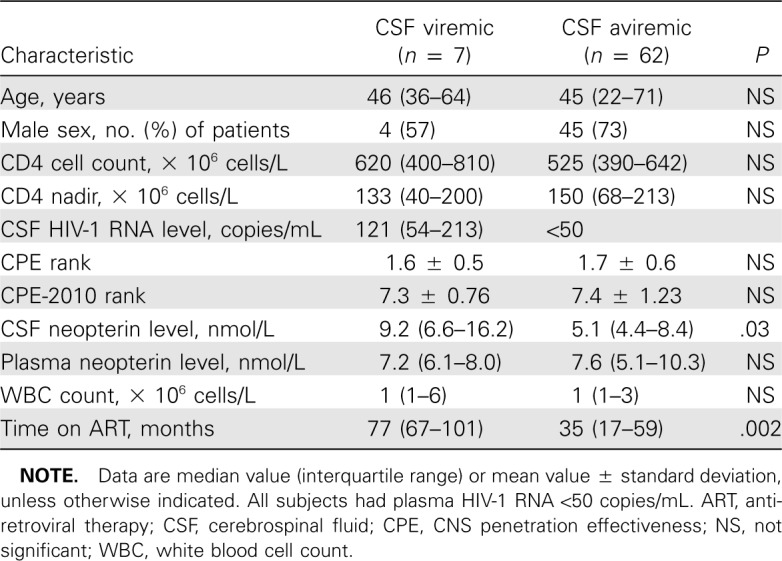
Results: Seven (10%) of the 69 subjects had detectable CSF HIV-1 RNA, in median 121 copies/mL (interquartile range, 54-213 copies/mL). Subjects with detectable CSF virus had significantly higher CSF neopterin and longer duration of treatment. Previous treatment interruptions were more common in subjects with CSF escape. Central nervous system penetration effectiveness rank was not a significant predictor of detectable CSF virus or CSF neopterin levels.
Conclusions: Viral escape in CSF is more common than previously reported, suggesting that low-grade central nervous system infection may continue in treated patients. Although these findings need extension in longitudinal studies, they suggest the utility of monitoring CSF responses, as new treatment combinations and strategies modify clinical practice.
Figures
Comment in
-
Viral escape in cerebrospinal fluid--an achilles heel of HIV therapy?J Infect Dis. 2010 Dec 15;202(12):1768-9. doi: 10.1086/657343. Epub 2010 Nov 4. J Infect Dis. 2010. PMID: 21050117 No abstract available.
-
Possibility of HIV-1 resistance mutations in cerebrospinal fluid from persons receiving suppressive therapy.J Infect Dis. 2011 Jul 1;204(1):174; author reply 174-5. doi: 10.1093/infdis/jir234. J Infect Dis. 2011. PMID: 21628673 Free PMC article. No abstract available.
References
-
- Gisslen M, Fuchs D, Svennerholm B, Hagberg L. Cerebrospinal fluid viral load, intrathecal immunoactivation, and cerebrospinal fluid monocytic cell count in HIV-1 infection. J Acquir Immune Defic Syndr. 1999;21:271–276. - PubMed
-
- Ellis RJ, Hsia K, Spector SA, et al. Cerebrospinal fluid human immunodeficiency virus type 1 RNA levels are elevated in neurocognitively impaired individuals with acquired immunodeficiency syndrome: HIV neurobehavioral research center group. Ann Neurol. 1997;42:679–688. - PubMed
-
- Price RW, Brew BJ. The AIDS dementia complex. J Infect Dis. 1988;158:1079–1083. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
