

Tooth loss and oral health-related quality of life: a systematic review and meta-analysis
- PMID: 21050499
- PMCID: PMC2992503
- DOI: 10.1186/1477-7525-8-126
Tooth loss and oral health-related quality of life: a systematic review and meta-analysis
Abstract
Background: It is increasingly recognized that the impact of disease on quality of life should be taken into account when assessing health status. It is likely that tooth loss, in most cases being a consequence of oral diseases, affects Oral Health-Related Quality of Life (OHRQoL). The aim of the present study is to systematically review the literature and to analyse the relationship between the number and location of missing teeth and oral health-related quality of life (OHRQoL). It was hypothesized that tooth loss is associated with an impairment of OHRQoL. Secondly, it was hypothesized that location and distribution of remaining teeth play an important role in this.
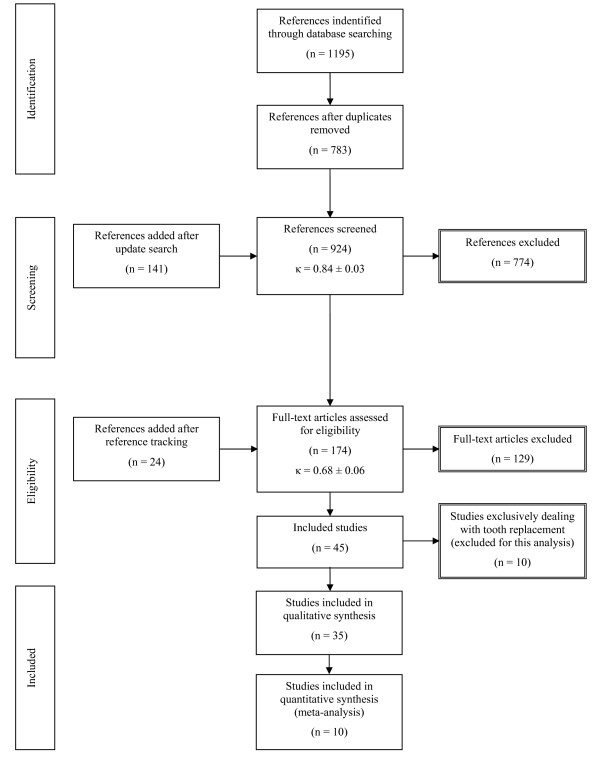
Methods: Relevant databases were searched for papers in English, published from 1990 to July 2009 following a broad search strategy. Relevant papers were selected by two independent readers using predefined exclusion criteria, firstly on the basis of abstracts, secondly by assessing full-text papers. Selected studies were grouped on the basis of OHRQoL instruments used and assessed for feasibility for quantitative synthesis. Comparable outcomes were subjected to meta-analysis; remaining outcomes were subjected to a qualitative synthesis only.
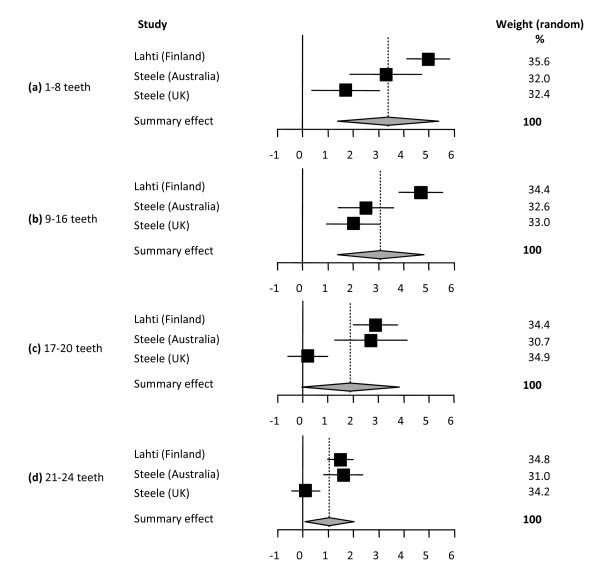
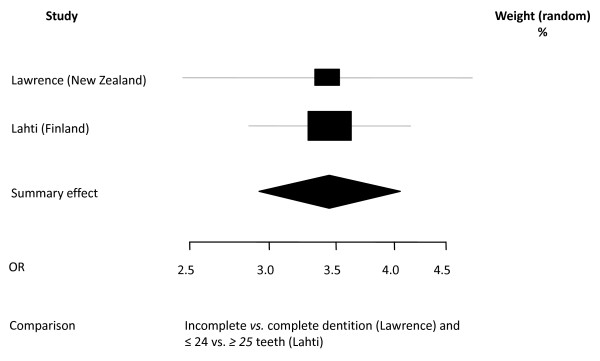
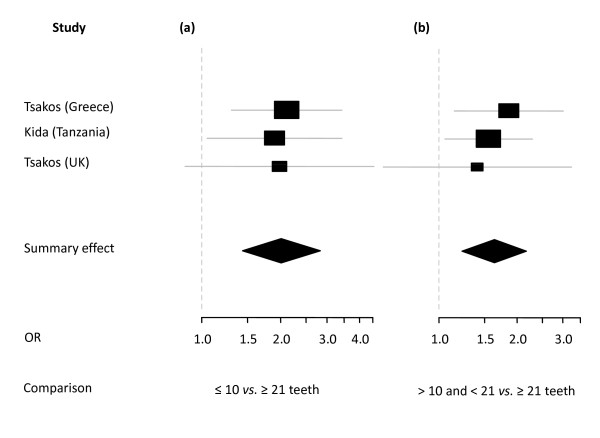
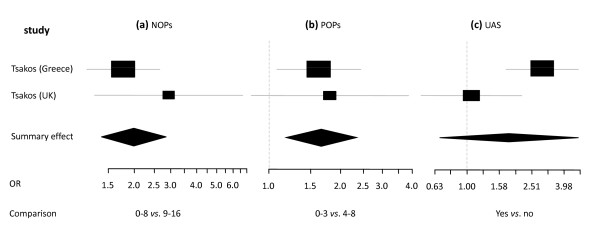
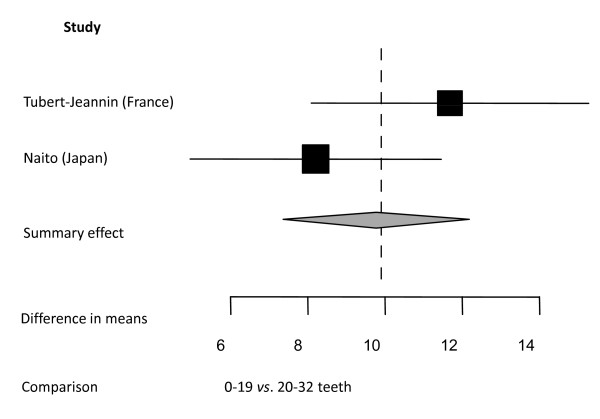
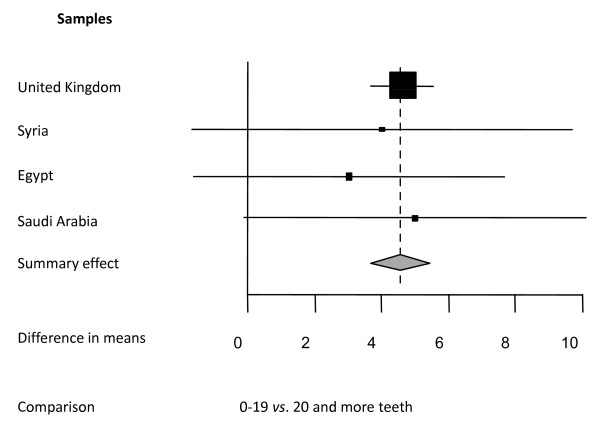
Results: From a total of 924 references, 35 were eligible for synthesis (inter-reader agreement abstracts κ = 0.84 ± 0.03; full-texts: κ = 0.68 ± 0.06). Meta-analysis was feasible for 10 studies reporting on 13 different samples, resulting in 6 separate analyses. All studies showed that tooth loss is associated with unfavourable OHRQoL scores, independent of study location and OHRQoL instrument used. Qualitative synthesis showed that all 9 studies investigating a possible relationship between number of occluding pairs of teeth present and OHRQoL reported significant positive correlations. Five studies presented separate data regarding OHRQoL and location of tooth loss (anterior tooth loss vs. posterior tooth loss). Four of these reported highest impact for anterior tooth loss; one study indicated a similar impact for both locations of tooth loss.
Conclusions: This study provides fairly strong evidence that tooth loss is associated with impairment of OHRQoL and location and distribution of tooth loss affect the severity of the impairment. This association seems to be independent from the OHRQoL instrument used and context of the included samples.
Figures
References
-
- Decker SD, Schultz R, Wood D. Determinants of well-being in primary caregivers of spinal cord injured persons. Rehabil Nurs. 1989;14:6–8. - PubMed
-
- Mack F, Schwahn C, Feine JS, Mundt T, Bernhardt O, John U, Kocher PT, Biffar R. The impact of tooth loss on general health related to quality of life among elderly Pomeranians: results from the study of health in Pomerania (SHIP-O) Int J Prosthodont. 2005;18:414–419. - PubMed
-
- Marino R, Schofield M, Wright C, Calache H, Minichiello V. Self-reported and clinically determined oral health status predictors for quality of life in dentate older migrant adults. Community Dent Oral Epidemiol. 2008;36:85–94. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
