

Staff acceptance of tele-ICU coverage: a systematic review
- PMID: 21051386
- PMCID: PMC3032369
- DOI: 10.1378/chest.10-1795
Staff acceptance of tele-ICU coverage: a systematic review
Abstract
Background: Remote coverage of ICUs is increasing, but staff acceptance of this new technology is incompletely characterized. We conducted a systematic review to summarize existing research on acceptance of tele-ICU coverage among ICU staff.
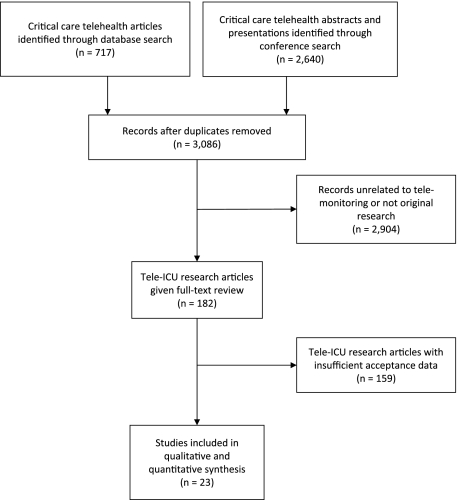
Methods: We searched for published articles pertaining to critical care telemedicine systems (aka, tele-ICU) between January 1950 and March 2010 using PubMed, Cumulative Index to Nursing and Allied Health Literature, Global Health, Web of Science, and the Cochrane Library and abstracts and presentations delivered at national conferences. Studies were included if they provided original qualitative or quantitative data on staff perceptions of tele-ICU coverage. Studies were imported into content analysis software and coded by tele-ICU configuration, methodology, participants, and findings (eg, positive and negative staff evaluations).
Results: Review of 3,086 citations yielded 23 eligible studies. Findings were grouped into four categories of staff evaluation: overall acceptance level of tele-ICU coverage (measured in 70% of studies), impact on patient care (measured in 96%), impact on staff (measured in 100%), and organizational impact (measured in 48%). Overall acceptance was high, despite initial ambivalence. Favorable impact on patient care was perceived by > 82% of participants. Staff impact referenced enhanced collaboration, autonomy, and training, although scrutiny, malfunctions, and contradictory advice were cited as potential barriers. Staff perceived the organizational impact to vary. An important limitation of available studies was a lack of rigorous methodology and validated survey instruments in many studies.
Conclusions: Initial reports suggest high levels of staff acceptance of tele-ICU coverage, but more rigorous methodologic study is required.
Figures
Similar articles
-
Impact of telemedicine intensive care unit coverage on patient outcomes: a systematic review and meta-analysis.Arch Intern Med. 2011 Mar 28;171(6):498-506. doi: 10.1001/archinternmed.2011.61. Arch Intern Med. 2011. PMID: 21444842
-
Centralized monitoring and virtual consultant models of tele-ICU care: a systematic review.Telemed J E Health. 2014 Oct;20(10):936-61. doi: 10.1089/tmj.2013.0352. Epub 2014 Sep 16. Telemed J E Health. 2014. PMID: 25226571
-
Factors that impact on the use of mechanical ventilation weaning protocols in critically ill adults and children: a qualitative evidence-synthesis.Cochrane Database Syst Rev. 2016 Oct 4;10(10):CD011812. doi: 10.1002/14651858.CD011812.pub2. Cochrane Database Syst Rev. 2016. PMID: 27699783 Free PMC article.
-
Eliciting adverse effects data from participants in clinical trials.Cochrane Database Syst Rev. 2018 Jan 16;1(1):MR000039. doi: 10.1002/14651858.MR000039.pub2. Cochrane Database Syst Rev. 2018. PMID: 29372930 Free PMC article.
-
The effectiveness of interventions to meet family needs of critically ill patients in an adult intensive care unit: a systematic review update.JBI Database System Rev Implement Rep. 2016 Mar;14(3):181-234. doi: 10.11124/JBISRIR-2016-2477. JBI Database System Rev Implement Rep. 2016. PMID: 27532144
Cited by
-
Review of Systematic Reviews in the Field of Telemedicine.Med J Islam Repub Iran. 2021 Dec 29;35:184. doi: 10.47176/mjiri.35.184. eCollection 2021. Med J Islam Repub Iran. 2021. PMID: 36042824 Free PMC article.
-
Barriers to patient and family-centred care in adult intensive care units: A systematic review.Nurs Open. 2019 Mar 28;6(3):676-684. doi: 10.1002/nop2.253. eCollection 2019 Jul. Nurs Open. 2019. PMID: 31367389 Free PMC article. Review.
-
Work System Barriers and Strategies Reported by Tele-Intensive Care Unit Nurses: A Case Study.Crit Care Nurs Clin North Am. 2018 Jun;30(2):259-271. doi: 10.1016/j.cnc.2018.02.008. Crit Care Nurs Clin North Am. 2018. PMID: 29724444 Free PMC article.
-
Impact of Information and Communication Technologies on Nursing Care: Results of an Overview of Systematic Reviews.J Med Internet Res. 2017 Apr 25;19(4):e122. doi: 10.2196/jmir.6686. J Med Internet Res. 2017. PMID: 28442454 Free PMC article.
-
The effect of telemedicine in critically ill patients: systematic review and meta-analysis.Crit Care. 2012 Jul 18;16(4):R127. doi: 10.1186/cc11429. Crit Care. 2012. PMID: 22809335 Free PMC article.
References
-
- Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA. 2002;288(17):2151–2162. - PubMed
-
- Duke EM. Report to Congress: The Critical Care Workforce: A Study of the Supply and Demand for Critical Care Physicians. Washington, DC: US Department of Health and Human Services HRSA; 2006.
-
- Gutsche JT, Kohl BA. Who should care for intensive care unit patients? Crit Care Med. 2007;35(2 suppl):S18–S23. - PubMed
-
- National Library of Medicine . National Library of Medicine: medical subject Headings. Bethesda, MD: National Library of Medicine; 2010.
-
- Berenson RA, Grossman JM, November EA. Does telemonitoring of patients—the eICU—improve intensive care? Health Aff (Millwood) 2009;28(5):w937–w947. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
