

Monitoring non-invasive cardiac output and stroke volume during experimental human hypovolaemia and resuscitation
- PMID: 21051492
- PMCID: PMC3000628
- DOI: 10.1093/bja/aeq295
Monitoring non-invasive cardiac output and stroke volume during experimental human hypovolaemia and resuscitation
Abstract
Background: Multiple methods for non-invasive measurement of cardiac output (CO) and stroke volume (SV) exist. Their comparative capabilities are not clearly established.
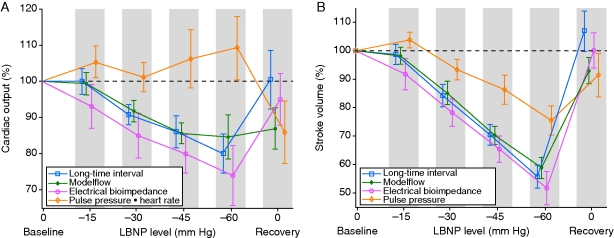
Methods: Healthy human subjects (n=21) underwent central hypovolaemia through progressive lower body negative pressure (LBNP) until the onset of presyncope, followed by termination of LBNP, to simulate complete resuscitation. Measurement methods were electrical bioimpedance (EBI) of the thorax and three measurements of CO and SV derived from the arterial blood pressure (ABP) waveform: the Modelflow (MF) method, the long-time interval (LTI) method, and pulse pressure (PP). We computed areas under receiver-operating characteristic curves (ROC AUCs) for the investigational metrics, to determine how well they discriminated between every combination of LBNP levels.
Results: LTI and EBI yielded similar reductions in SV during progressive hypovolaemia and resuscitation (correlation coefficient 0.83) with ROC AUCs for distinguishing major LBNP (-60 mm Hg) vs resuscitation (0 mm Hg) of 0.98 and 0.99, respectively. MF yielded very similar reductions and ROC AUCs during progressive hypovolaemia, but after resuscitation, MF-CO did not return to baseline, yielding lower ROC AUCs (ΔROC AUC range, -0.18 to -0.26, P < 0.01). PP declined during hypovolaemia but tended to be an inferior indicator of specific LBNP levels, and PP did not recover during resuscitation, yielding lower ROC curves (P < 0.01).
Conclusions: LTI, EBI, and MF were able to track progressive hypovolaemia. PP decreased during hypovolaemia but its magnitude of reduction underestimated reductions in SV. PP and MF were inferior for the identification of resuscitation.
Figures
Similar articles
-
Comparison of cardiac output monitoring methods for detecting central hypovolemia due to lower body negative pressure.Annu Int Conf IEEE Eng Med Biol Soc. 2007;2007:955-8. doi: 10.1109/IEMBS.2007.4352450. Annu Int Conf IEEE Eng Med Biol Soc. 2007. PMID: 18002116
-
Tracking central hypovolemia with ecg in humans: cautions for the use of heart period variability in patient monitoring.Shock. 2010 Jun;33(6):583-9. doi: 10.1097/SHK.0b013e3181cd8cbe. Shock. 2010. PMID: 19997052
-
Arterial pulse pressure and its association with reduced stroke volume during progressive central hypovolemia.J Trauma. 2006 Sep;61(3):629-34. doi: 10.1097/01.ta.0000196663.34175.33. J Trauma. 2006. PMID: 16966999
-
Lightweight noninvasive trauma monitor for early indication of central hypovolemia and tissue acidosis: a review.J Trauma Acute Care Surg. 2012 Aug;73(2 Suppl 1):S106-11. doi: 10.1097/TA.0b013e318260a928. J Trauma Acute Care Surg. 2012. PMID: 22847078 Review.
-
Recognizing hypovolaemia.Minerva Anestesiol. 2001 Apr;67(4):185-9. Minerva Anestesiol. 2001. PMID: 11376507 Review.
Cited by
-
Capability of a new paediatric oesophageal Doppler monitor to detect changes in cardiac output during testing of external pacemakers after cardiac surgery.J Clin Monit Comput. 2011 Dec;25(6):419-25. doi: 10.1007/s10877-011-9322-0. Epub 2011 Nov 12. J Clin Monit Comput. 2011. PMID: 22081259
-
Cardiac output estimation using multi-beat analysis of the radial arterial blood pressure waveform: a method comparison study in patients having off-pump coronary artery bypass surgery using intermittent pulmonary artery thermodilution as the reference method.J Clin Monit Comput. 2020 Aug;34(4):649-654. doi: 10.1007/s10877-019-00375-z. Epub 2019 Aug 27. J Clin Monit Comput. 2020. PMID: 31456072 Free PMC article.
-
Using the Pulse Contour Method to Measure the Changes in Stroke Volume during a Passive Leg Raising Test.Sensors (Basel). 2018 Oct 12;18(10):3420. doi: 10.3390/s18103420. Sensors (Basel). 2018. PMID: 30322018 Free PMC article.
-
Quantification of stroke volume in a simulated healthy volunteer model of traumatic haemorrhage; a comparison of two non-invasive monitoring devices using error grid analysis alongside traditional measures of agreement.PLoS One. 2021 Dec 23;16(12):e0261546. doi: 10.1371/journal.pone.0261546. eCollection 2021. PLoS One. 2021. PMID: 34941918 Free PMC article.
-
Comparison of compensatory reserve during lower-body negative pressure and hemorrhage in nonhuman primates.Am J Physiol Regul Integr Comp Physiol. 2016 Jun 1;310(11):R1154-9. doi: 10.1152/ajpregu.00304.2015. Epub 2016 Mar 30. Am J Physiol Regul Integr Comp Physiol. 2016. PMID: 27030667 Free PMC article.
References
-
- Parks JK, Elliott AC, Gentilello LM, Shafi S. Systemic hypotension is a late marker of shock after trauma: a validation study of Advanced Trauma Life Support principles in a large national sample. Am J Surg. 2006;192:727–31. - PubMed
-
- Convertino VA, Ryan KL, Rickards CA, et al. Physiological and medical monitoring for en route care of combat casualties. J Trauma. 2008;64:S342–53. - PubMed
-
- Snyder HS, Dresnick SJ. Lack of tachycardic response to hypotension in penetrating abdominal injuries. J Emerg Med. 1989;7:335–9. - PubMed
-
- Victorino GP, Battistella FD, Wisner DH. Does tachycardia correlate with hypotension after trauma? J Am Coll Surg. 2003;196:679–84. - PubMed
-
- Porter JM. The search for an optimal end point of resuscitation. J Trauma. 2000;48:360. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
