

Monitoring non-invasive cardiac output and stroke volume during experimental human hypovolaemia and resuscitation
- PMID: 21051492
- PMCID: PMC3000628
- DOI: 10.1093/bja/aeq295
Monitoring non-invasive cardiac output and stroke volume during experimental human hypovolaemia and resuscitation
Abstract
Background: Multiple methods for non-invasive measurement of cardiac output (CO) and stroke volume (SV) exist. Their comparative capabilities are not clearly established.
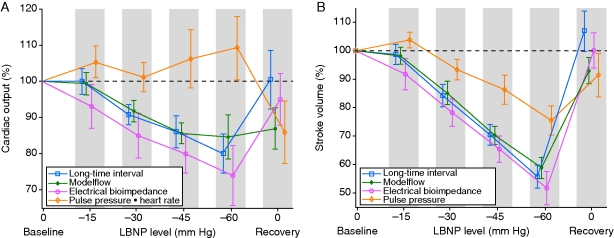
Methods: Healthy human subjects (n=21) underwent central hypovolaemia through progressive lower body negative pressure (LBNP) until the onset of presyncope, followed by termination of LBNP, to simulate complete resuscitation. Measurement methods were electrical bioimpedance (EBI) of the thorax and three measurements of CO and SV derived from the arterial blood pressure (ABP) waveform: the Modelflow (MF) method, the long-time interval (LTI) method, and pulse pressure (PP). We computed areas under receiver-operating characteristic curves (ROC AUCs) for the investigational metrics, to determine how well they discriminated between every combination of LBNP levels.
Results: LTI and EBI yielded similar reductions in SV during progressive hypovolaemia and resuscitation (correlation coefficient 0.83) with ROC AUCs for distinguishing major LBNP (-60 mm Hg) vs resuscitation (0 mm Hg) of 0.98 and 0.99, respectively. MF yielded very similar reductions and ROC AUCs during progressive hypovolaemia, but after resuscitation, MF-CO did not return to baseline, yielding lower ROC AUCs (ΔROC AUC range, -0.18 to -0.26, P < 0.01). PP declined during hypovolaemia but tended to be an inferior indicator of specific LBNP levels, and PP did not recover during resuscitation, yielding lower ROC curves (P < 0.01).
Conclusions: LTI, EBI, and MF were able to track progressive hypovolaemia. PP decreased during hypovolaemia but its magnitude of reduction underestimated reductions in SV. PP and MF were inferior for the identification of resuscitation.
Figures
References
-
- Parks JK, Elliott AC, Gentilello LM, Shafi S. Systemic hypotension is a late marker of shock after trauma: a validation study of Advanced Trauma Life Support principles in a large national sample. Am J Surg. 2006;192:727–31. - PubMed
-
- Convertino VA, Ryan KL, Rickards CA, et al. Physiological and medical monitoring for en route care of combat casualties. J Trauma. 2008;64:S342–53. - PubMed
-
- Snyder HS, Dresnick SJ. Lack of tachycardic response to hypotension in penetrating abdominal injuries. J Emerg Med. 1989;7:335–9. - PubMed
-
- Victorino GP, Battistella FD, Wisner DH. Does tachycardia correlate with hypotension after trauma? J Am Coll Surg. 2003;196:679–84. - PubMed
-
- Porter JM. The search for an optimal end point of resuscitation. J Trauma. 2000;48:360. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
