

Consistent changes in intracranial pressure waveform morphology induced by acute hypercapnic cerebral vasodilatation
- PMID: 21052864
- PMCID: PMC3130848
- DOI: 10.1007/s12028-010-9463-x
Consistent changes in intracranial pressure waveform morphology induced by acute hypercapnic cerebral vasodilatation
Abstract
Background: Intracranial pressure (ICP) remains a pivotal physiological signal for managing brain injury and subarachnoid hemorrhage (SAH) patients in neurocritical care units. Given the vascular origin of the ICP, changes in ICP waveform morphology could be used to infer cerebrovascular changes. Clinical validation of this association in the setting of brain trauma, and SAH is challenging due to the multi-factorial influences on, and uncertainty of, the state of the cerebral vasculature.
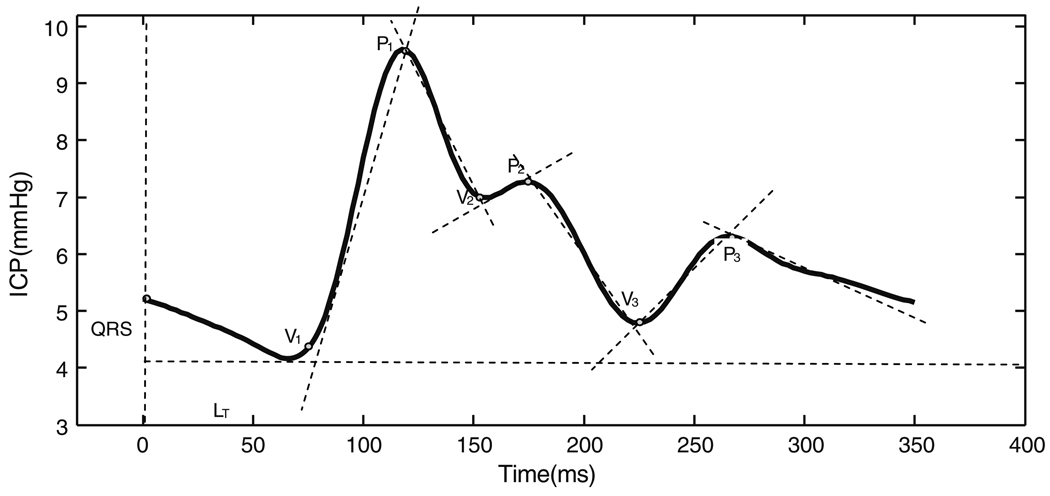
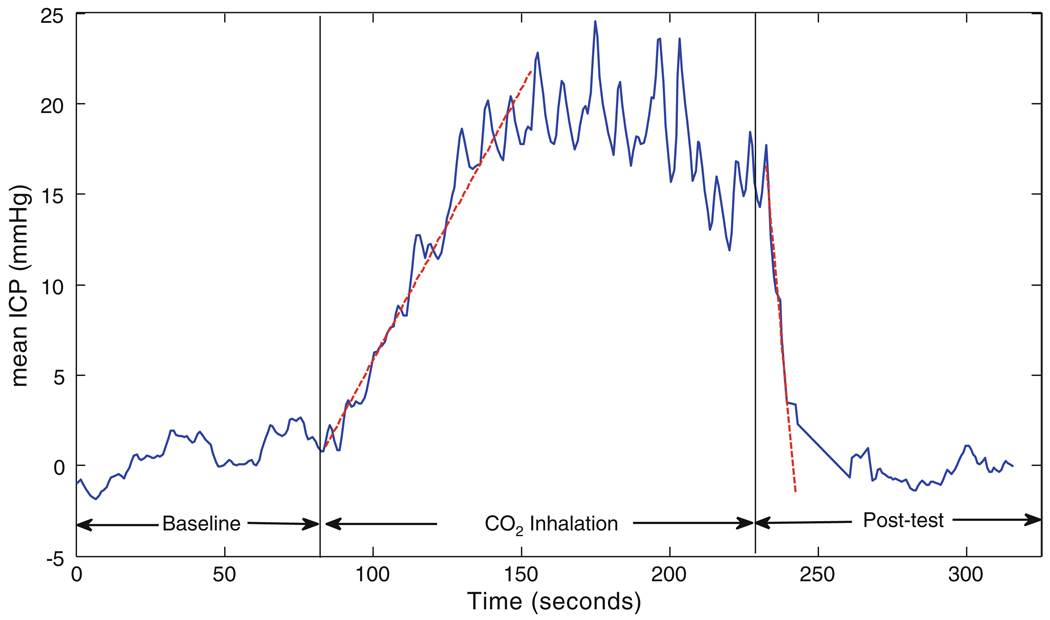
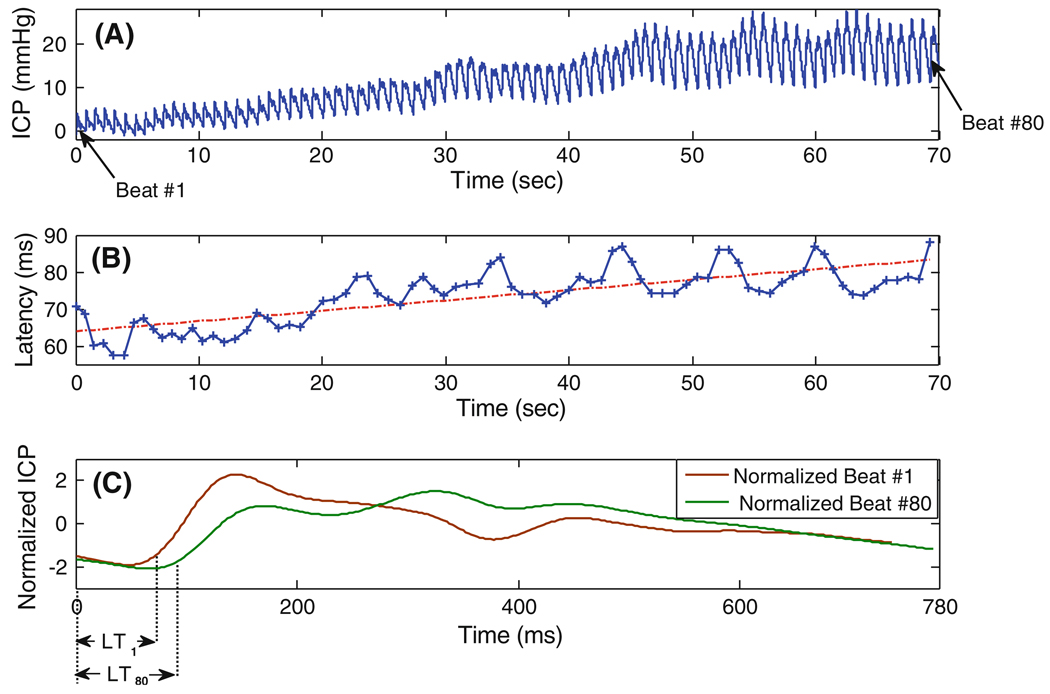
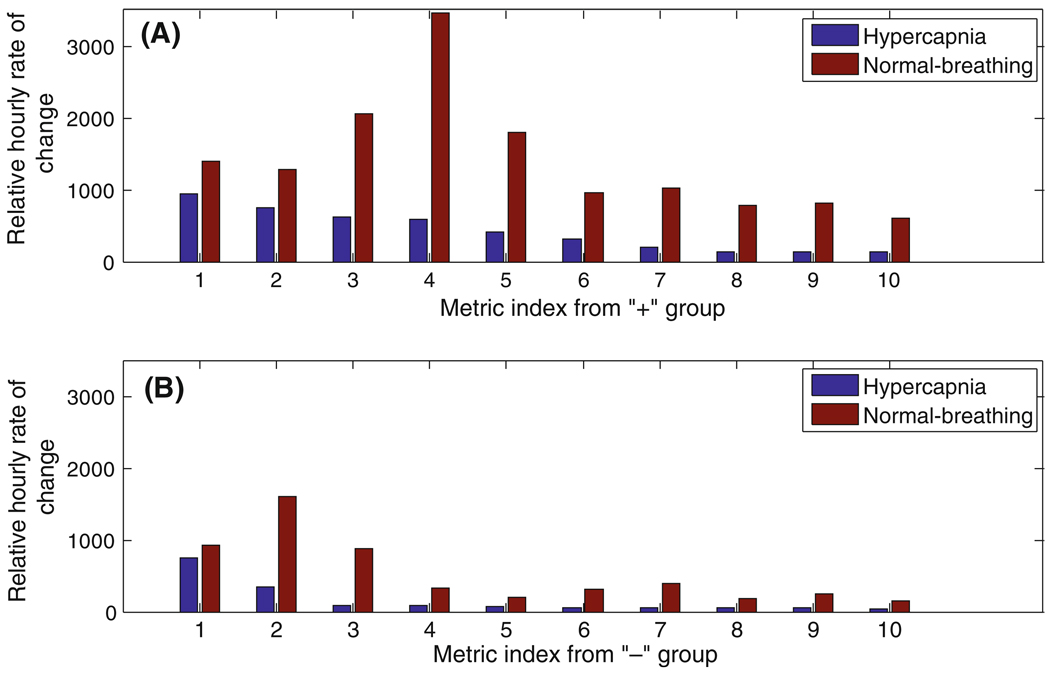
Methods: To gain a more controlled setting, in this articel, we study ICP signals recorded in four uninjured patients undergoing a CO2 inhalation challenge in which hypercapnia induced acute cerebral vasodilatation. We apply our morphological clustering and analysis of intracranial pressure (MOCAIP) algorithm to identify six landmarks on individual ICP pulses (based on the three established ICP sub-peaks; P1, P2, and P3) and extract 128 ICP morphological metrics. Then by comparing baseline, test, and post-test data, we assess the consistency and rate of change for each individual metric.
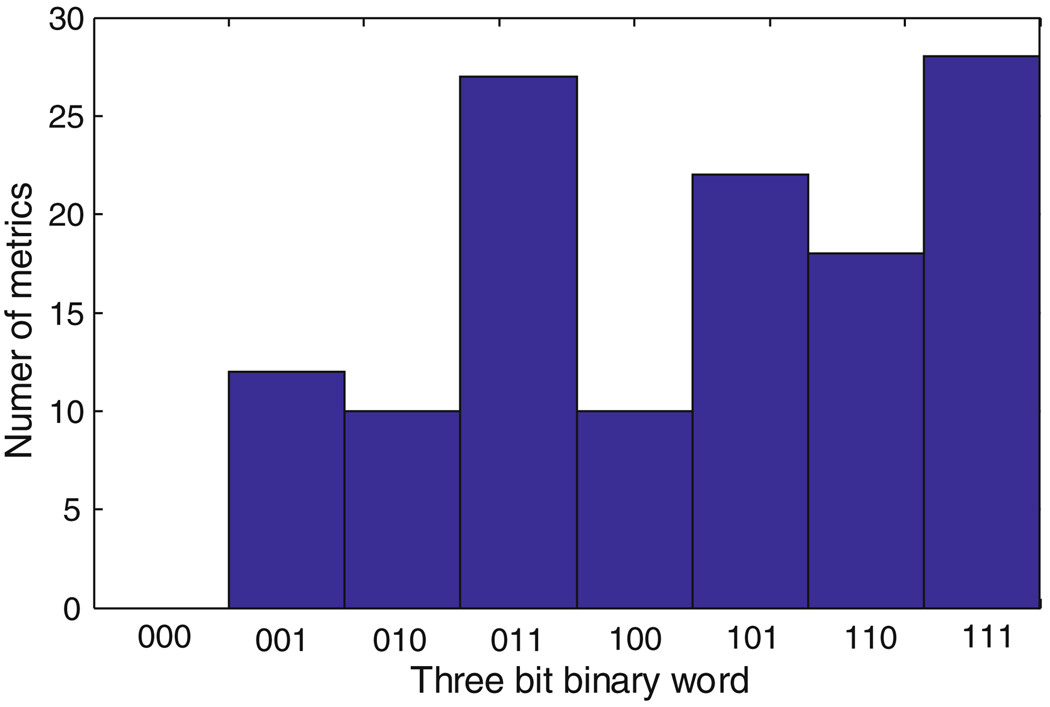
Results: Acute vasodilatation causes consistent changes in a total of 72 ICP pulse morphological metrics and the P2 sub-region responds to cerebral vascular changes in the most consistent way with the greatest change as compared to P1 and P3 sub-regions.
Conclusions: Since the dilation/constriction of the cerebral vasculature resulted in detectable consistent changes in ICP MOCIAP metrics, by an extended monitoring practice of ICP that includes characterizing ICP pulse morphology, one can potentially detect cerebrovascular changes, continuously, for patients under neurocritical care.
Figures
References
-
- Rao V, Lyketsos C. Neuropsychiatric sequelae of traumatic brain injury. Psychosomatics. 2000;41(2):95–103. - PubMed
-
- Brown AW, Elovic EP, Kothari S, Flanagan SR, Kwasnica C. Congenital and acquired brain injury. 1. Epidemiology, pathophysiology, prognostication, innovative treatments, and prevention. Arch Phys Med Rehabil. 2008;89(3) Suppl 1:S3–S8. - PubMed
-
- Fan JY, Kirkness C, Vicini P, Burr R, Mitchell P. Intracranial pressure waveform morphology and intracranial adaptive capacity. Am J Crit Care. 2008;17(6):545–554. - PubMed
-
- North B. Itracranial pressure monitoring. In: Reilly P, Bullock R, editors. Head injury: pathophysiology and management. Landon: Chapman & Hall Medical; 1997. pp. 209–216.
-
- March K, Mitchell P, Grady S, Winn R. Effect of backrest position on intracranial and cerebral perfusion pressures. J Neurosci Nurs. 1990;22(6):375–381. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
