

Revisiting human IL-12Rβ1 deficiency: a survey of 141 patients from 30 countries
- PMID: 21057261
- PMCID: PMC3129625
- DOI: 10.1097/MD.0b013e3181fdd832
Revisiting human IL-12Rβ1 deficiency: a survey of 141 patients from 30 countries
Abstract
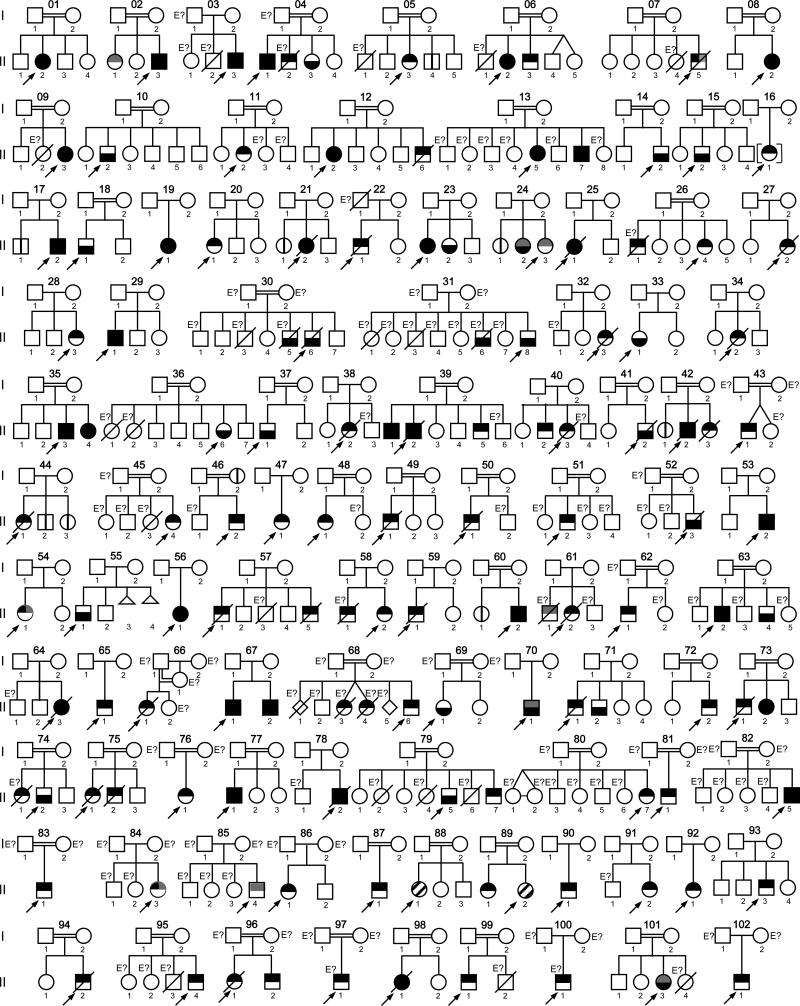
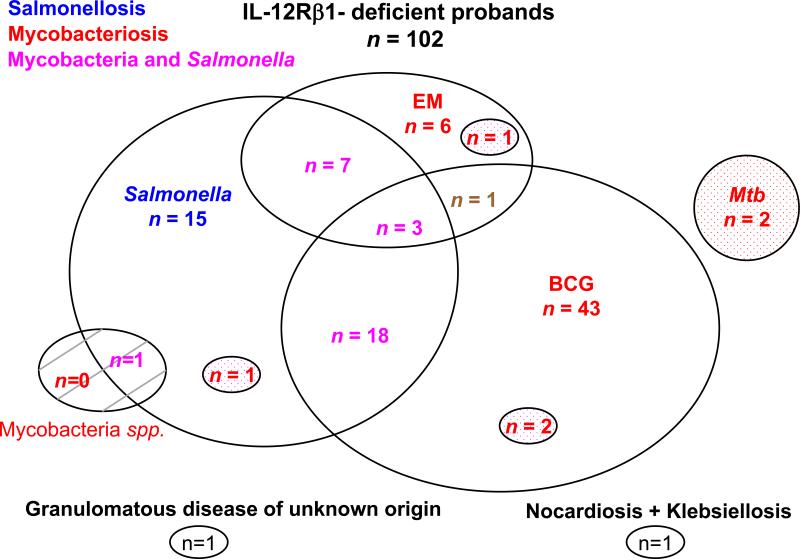
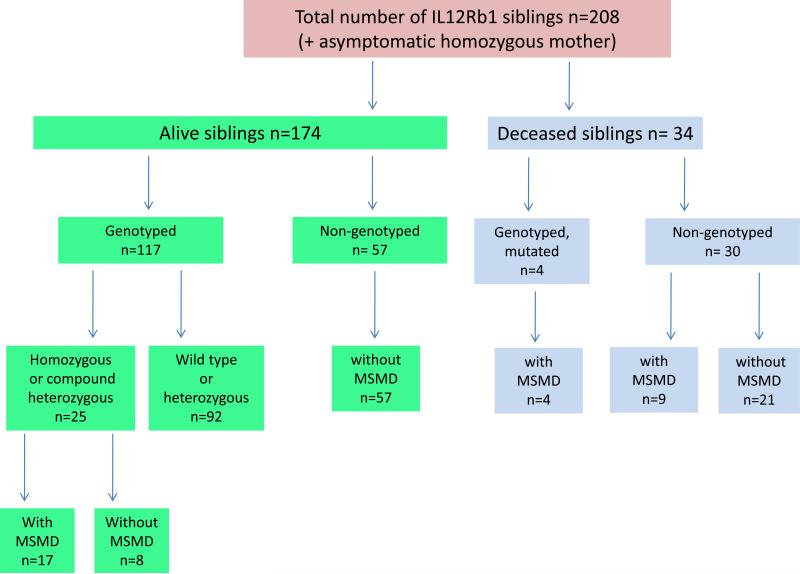
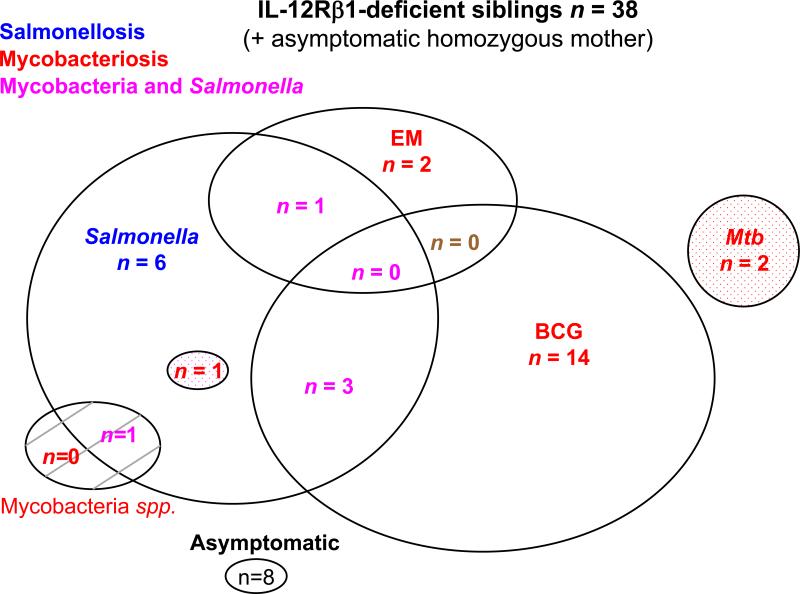
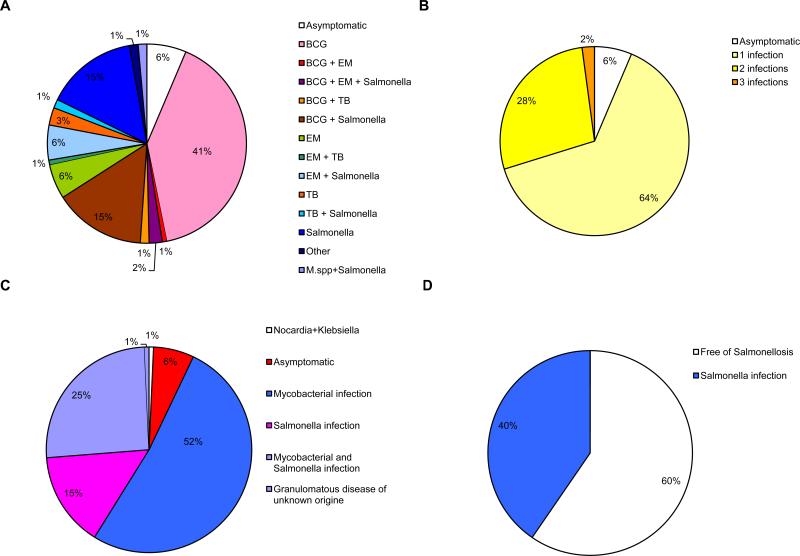
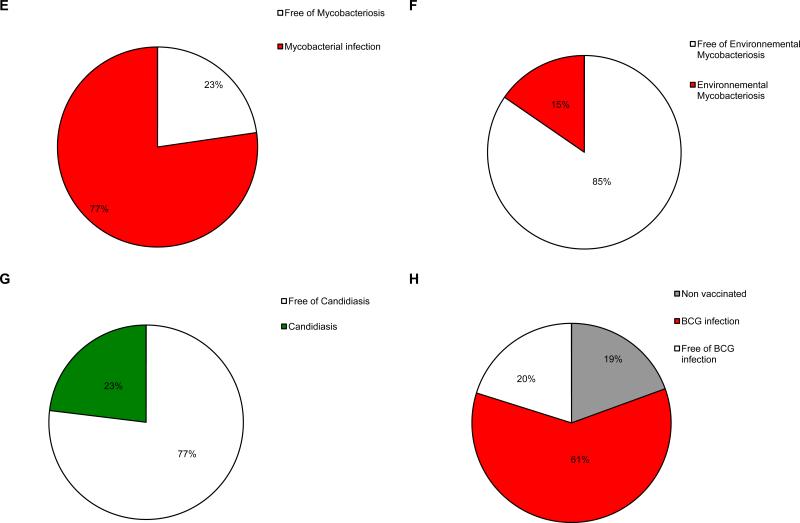
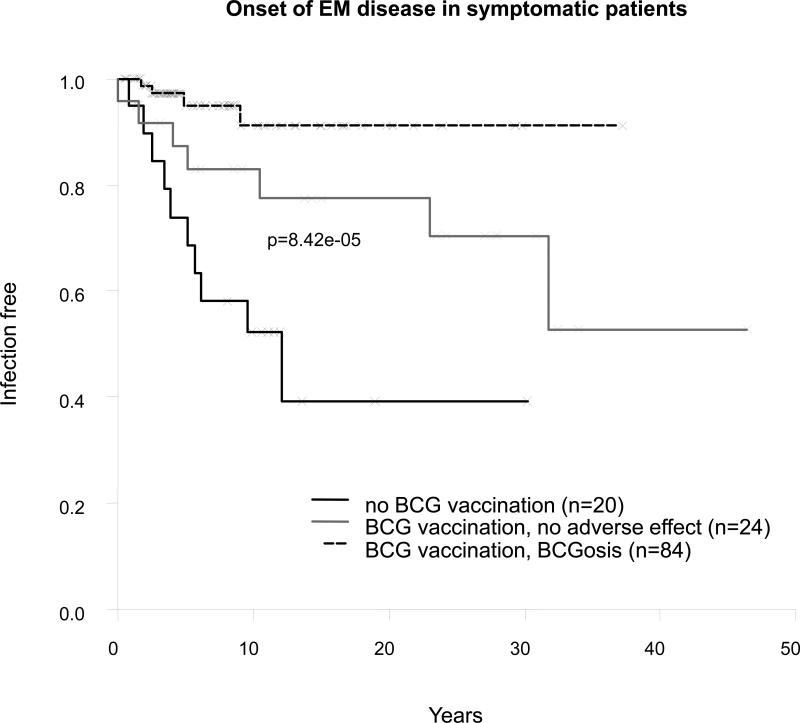
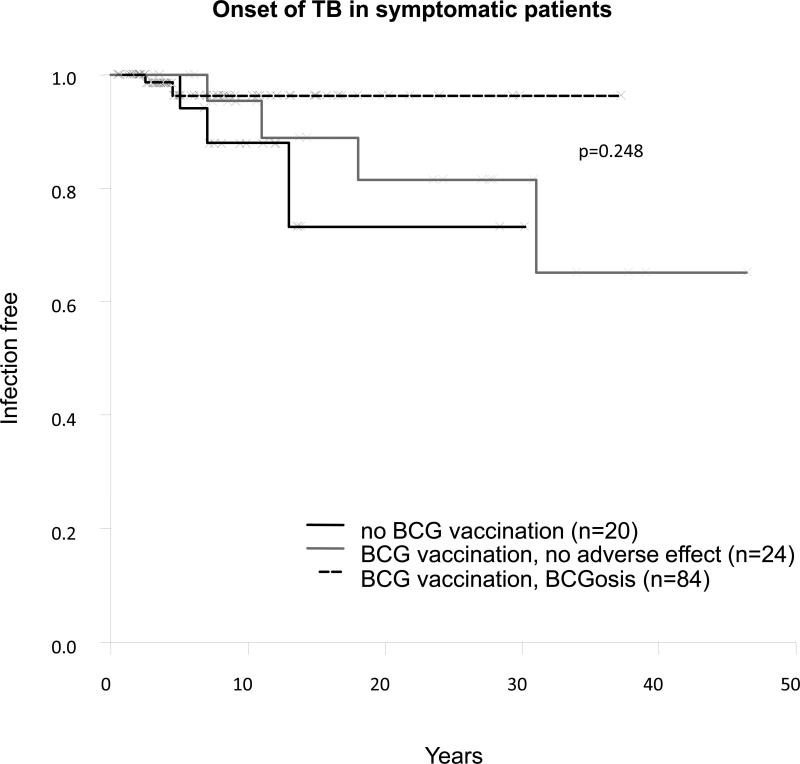
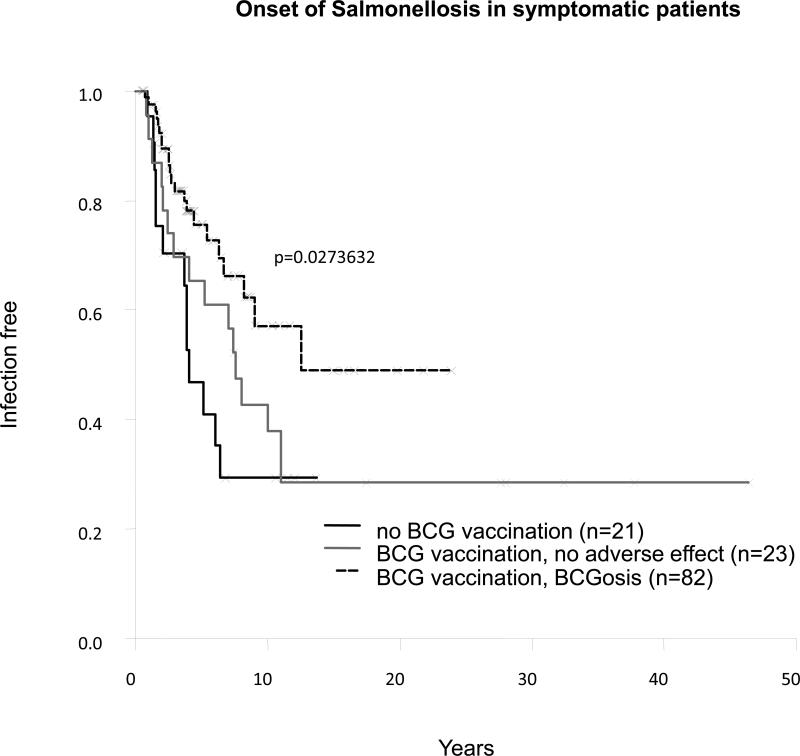
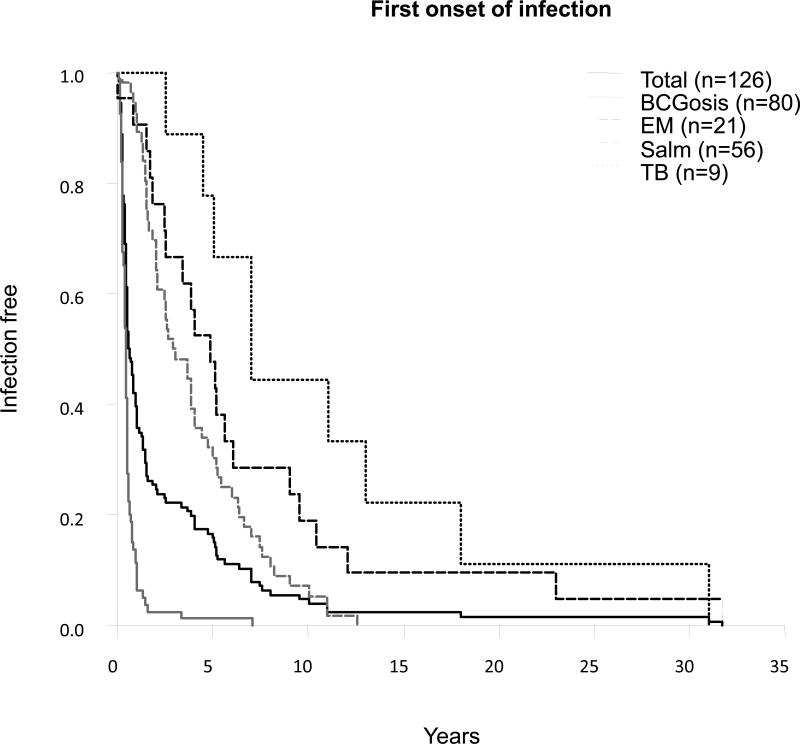
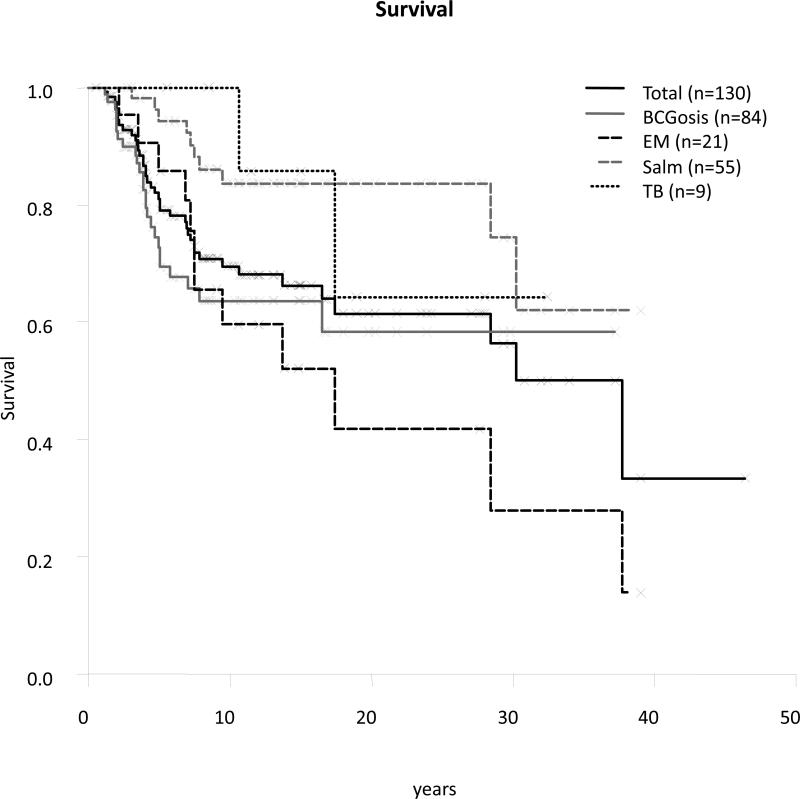
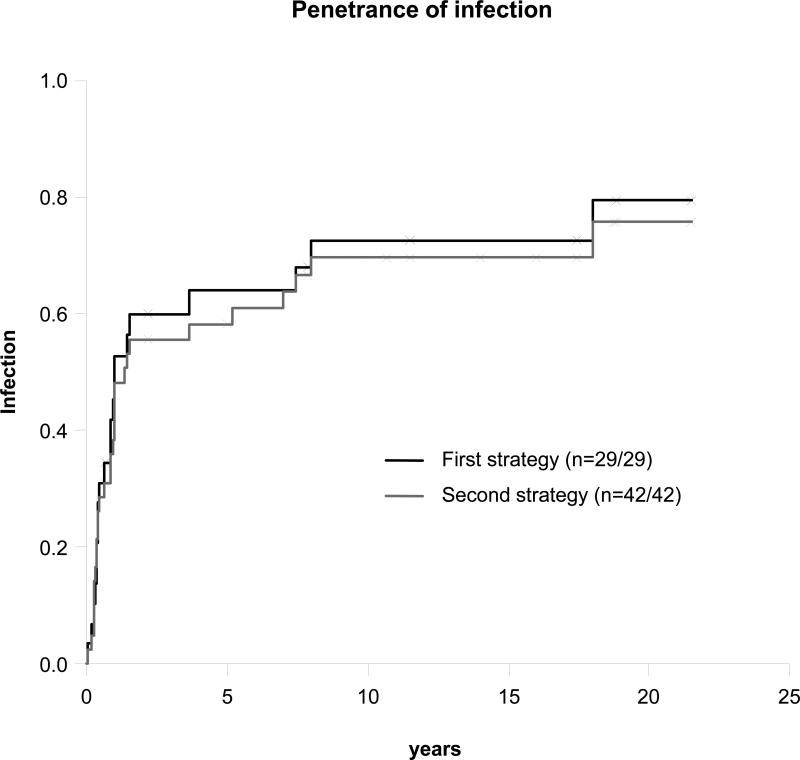
Interleukin-12 receptor β1 (IL-12Rβ1) deficiency is the most common form of Mendelian susceptibility to mycobacterial disease (MSMD). We undertook an international survey of 141 patients from 102 kindreds in 30 countries. Among 102 probands, the first infection occurred at a mean age of 2.4 years. In 78 patients, this infection was caused by Bacille Calmette-Guérin (BCG; n = 65), environmental mycobacteria (EM; also known as atypical or nontuberculous mycobacteria) (n = 9) or Mycobacterium tuberculosis (n = 4). Twenty-two of the remaining 24 probands initially presented with nontyphoidal, extraintestinal salmonellosis. Twenty of the 29 genetically affected sibs displayed clinical signs (69%); however 8 remained asymptomatic (27%). Nine nongenotyped sibs with symptoms died. Recurrent BCG infection was diagnosed in 15 cases, recurrent EM in 3 cases, recurrent salmonellosis in 22 patients. Ninety of the 132 symptomatic patients had infections with a single microorganism. Multiple infections were diagnosed in 40 cases, with combined mycobacteriosis and salmonellosis in 36 individuals. BCG disease strongly protected against subsequent EM disease (p = 0.00008). Various other infectious diseases occurred, albeit each rarely, yet candidiasis was reported in 33 of the patients (23%). Ninety-nine patients (70%) survived, with a mean age at last follow-up visit of 12.7 years ± 9.8 years (range, 0.5-46.4 yr). IL-12Rβ1 deficiency is characterized by childhood-onset mycobacteriosis and salmonellosis, rare recurrences of mycobacterial disease, and more frequent recurrence of salmonellosis. The condition has higher clinical penetrance, broader susceptibility to infections, and less favorable outcome than previously thought.
Figures
References
-
- Acosta-Rodriguez EV, Napolitani G, Lanzavecchia A, Sallusto F. Interleukins 1beta and 6 but not transforming growth factor-beta are essential for the differentiation of interleukin 17-producing human T helper cells. Nat Immunol. 2007;8:942–949. - PubMed
-
- Aksu G, Tirpan C, Cavusoglu C, Soydan S, Altare F, Casanova JL, Kutukculer N. Mycobacterium fortuitum-chelonae complex infection in a child with complete interleukin-12 receptor beta 1 deficiency. Pediatr Infect Dis J. 2001;20:551–553. - PubMed
-
- Al-Muhsen S, Casanova JL. The genetic heterogeneity of Mendelian susceptibility to mycobacterial diseases. J Allergy Clin Immunol. 2008;122:1043–1051. - PubMed
-
- Altare F, Durandy A, Lammas D, Emile JF, Lamhamedi S, Le Deist F, Drysdale P, Jouanguy E, Doffinger R, Bernaudin F, Jeppsson O, Gollob JA, Meinl E, Segal AW, Fischer A, Kumararatne D, Casanova JL. Impairment of mycobacterial immunity in human interleukin-12 receptor deficiency. Science. 1998;280:1432–1435. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
