

Vision therapy in adults with convergence insufficiency: clinical and functional magnetic resonance imaging measures
- PMID: 21057347
- PMCID: PMC3134155
- DOI: 10.1097/OPX.0b013e3181fef1aa
Vision therapy in adults with convergence insufficiency: clinical and functional magnetic resonance imaging measures
Abstract
Purpose: This research quantified clinical measurements and functional neural changes associated with vision therapy in subjects with convergence insufficiency (CI).
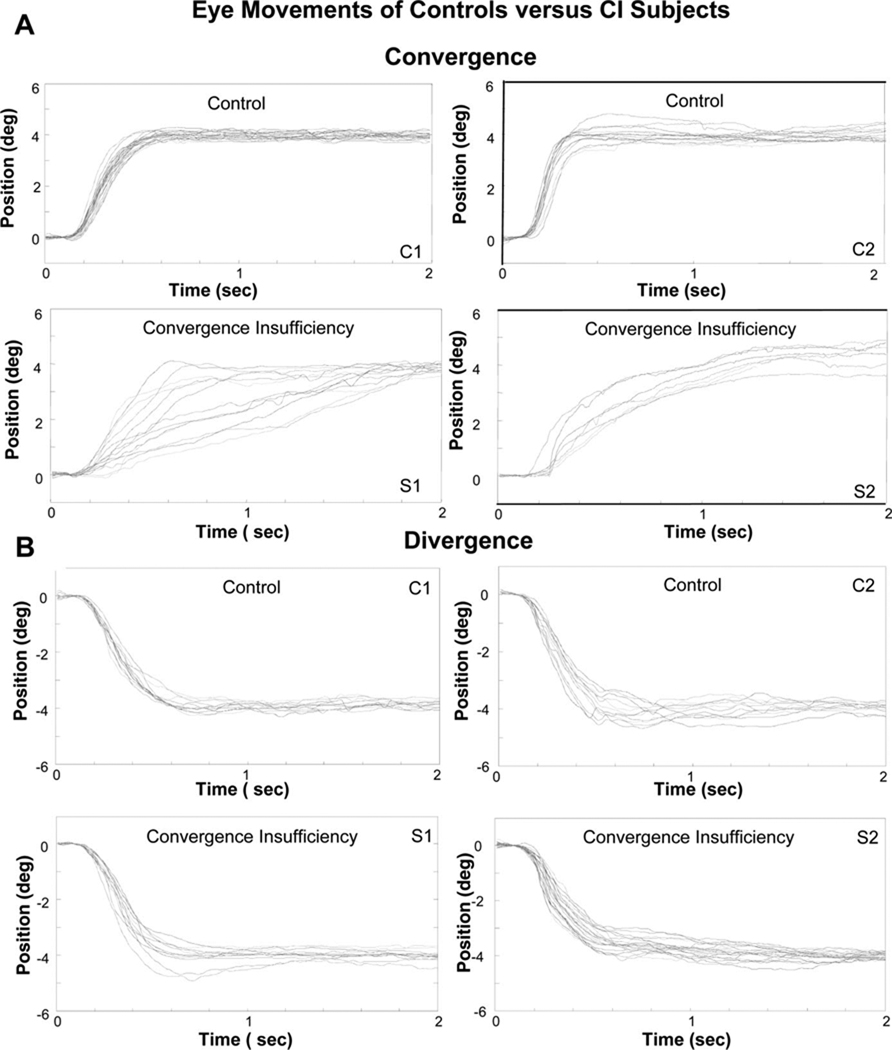
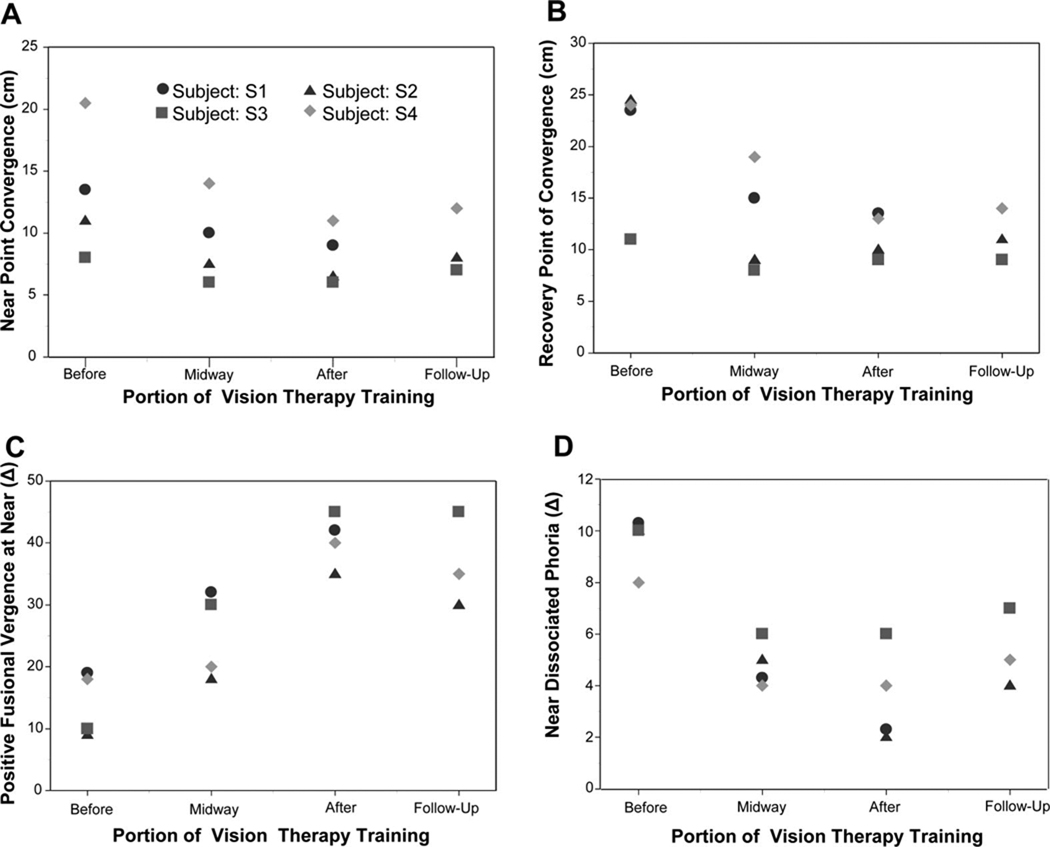
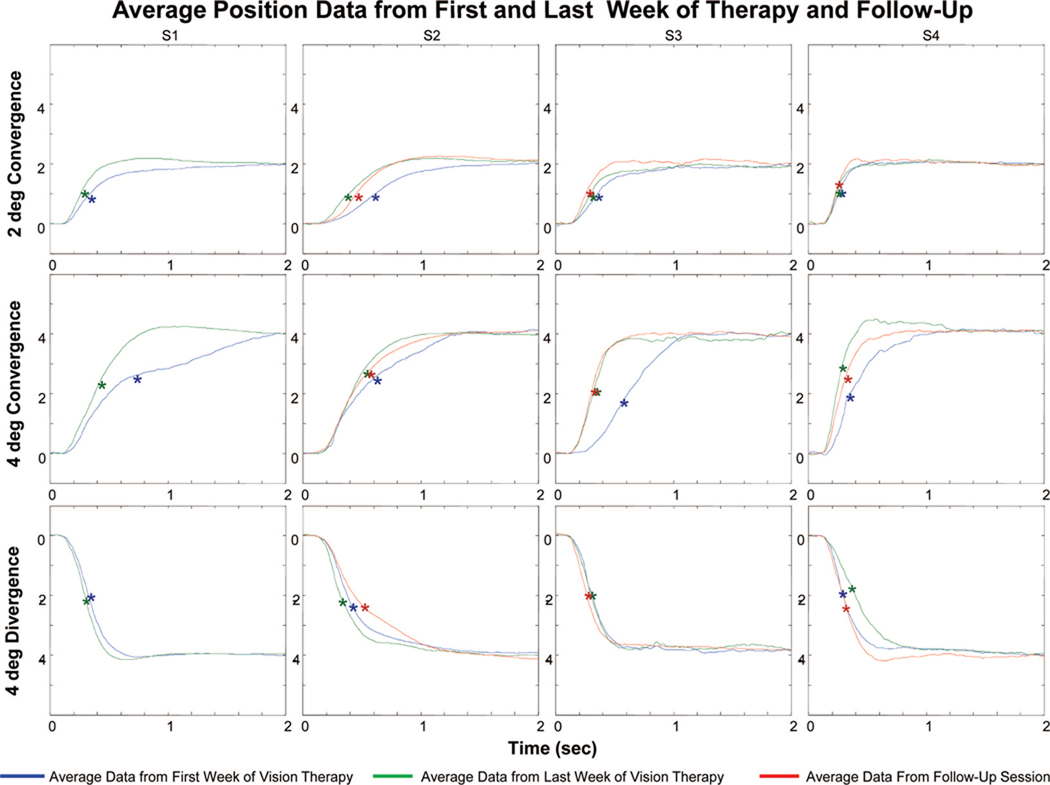
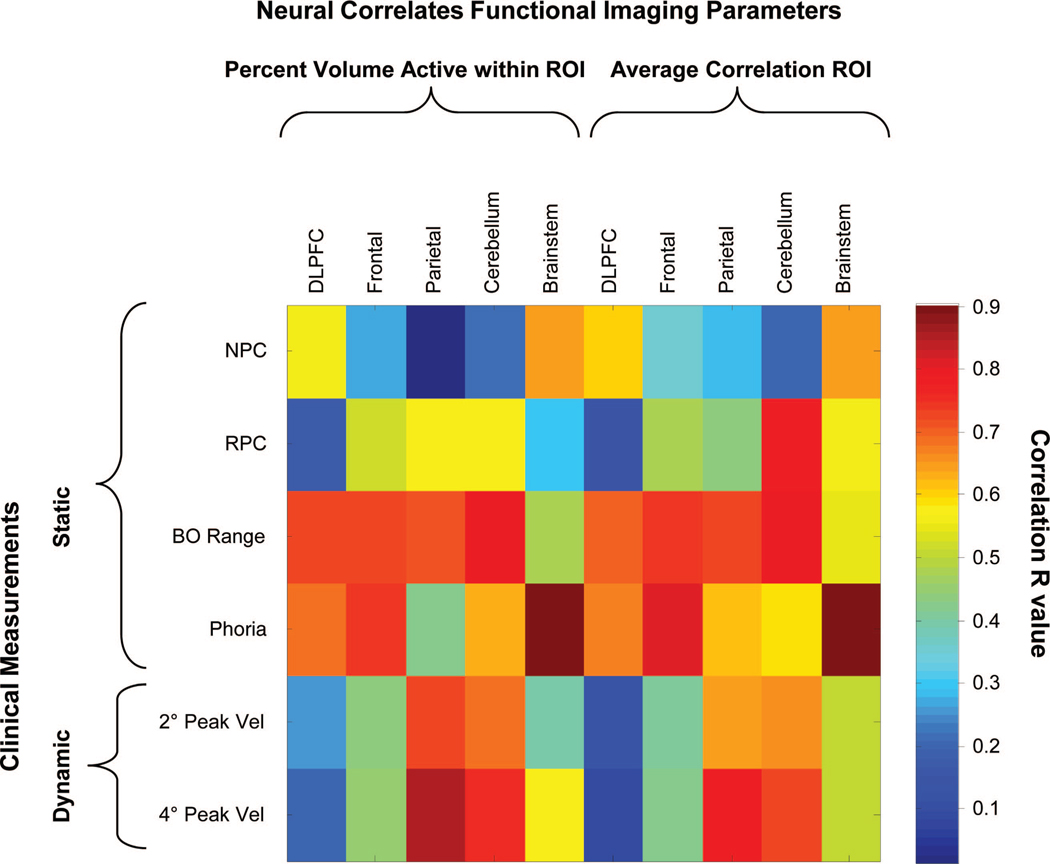
Methods: Convergence and divergence 4° step responses were compared between 13 control adult subjects with normal binocular vision and four CI adult subjects. All CI subjects participated in 18 h of vision therapy. Clinical parameters quantified throughout the therapy included: nearpoint of convergence, recovery point of convergence, positive fusional vergence at near, near dissociated phoria, and eye movements that were quantified using peak velocity. Neural correlates of the CI subjects were quantified with functional magnetic resonance imaging scans comparing random vs. predictable vergence movements using a block design before and after vision therapy. Images were quantified by measuring the spatial extent of activation and the average correlation within five regions of interests (ROI). The ROIs were the dorsolateral prefrontal cortex, a portion of the frontal lobe, part of the parietal lobe, the cerebellum, and the brain stem. All measurements were repeated 4 months to 1 year post-therapy in three of the CI subjects.
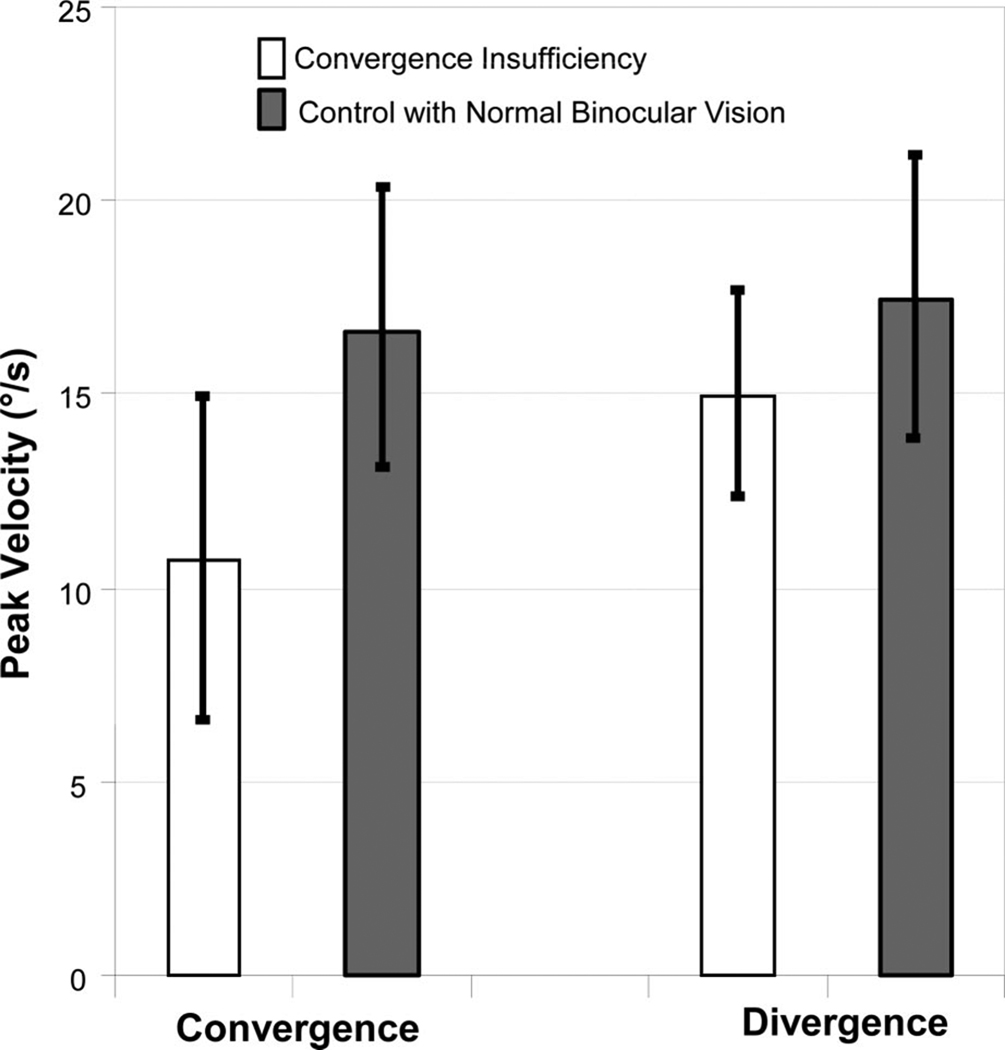
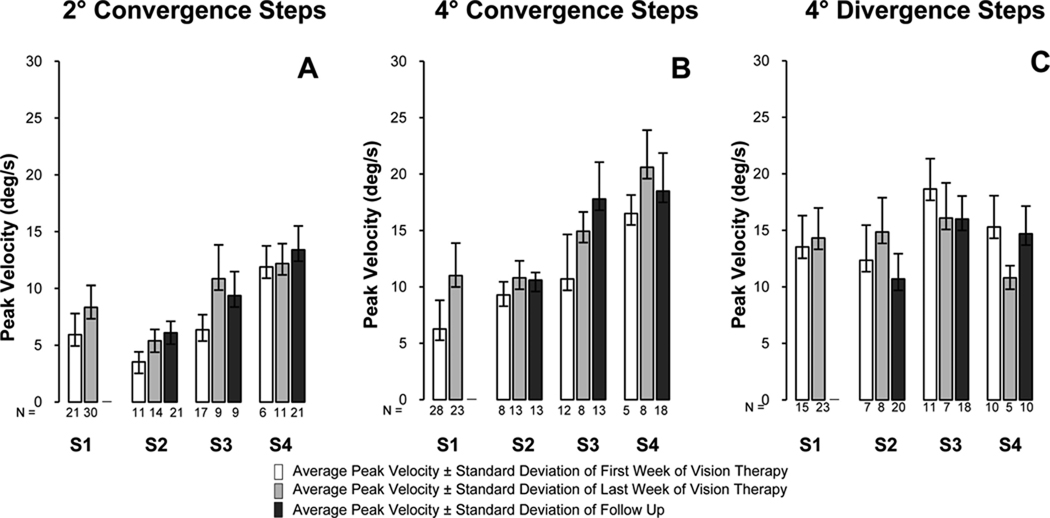
Results: Convergence average peak velocities to step stimuli were significantly slower (p = 0.016) in CI subjects compared with controls; however, significant differences in average peak velocities were not observed for divergence step responses (p = 0.30). The investigation of CI subjects participating in vision therapy showed that the nearpoint of convergence, recovery point of convergence, and near dissociated phoria significantly decreased. Furthermore, the positive fusional vergence, average peak velocity from 4° convergence steps, and the amount of functional activity within the frontal areas, cerebellum, and brain stem significantly increased. Several clinical and cortical parameters were significantly correlated.
Conclusions: Convergence peak velocity was significantly slower in CI subjects compared with controls, which may result in asthenopic complaints reported by the CI subjects. Vision therapy was associated with and may have evoked clinical and cortical activity changes.
Conflict of interest statement
None of the authors within this manuscript have commercial associations with the research that could result in a conflict of interest.
Figures



References
-
- Rouse MW, Hyman L, Hussein M, Solan H. Frequency of convergence insufficiency in optometry clinic settings. Convergence Insufficiency and Reading Study (CIRS) Group. Optom Vis Sci. 1998;75:88–96. - PubMed
-
- Scheiman M, Gallaway M, Coulter R, Reinstein F, Ciner E, Herzberg C, Parisi M. Prevalence of vision and ocular disease conditions in a clinical pediatric population. J Am Optom Assoc. 1996;67:193–202. - PubMed
-
- Rouse MW, Borsting E, Hyman L, Hussein M, Cotter SA, Flynn M, Scheiman M, Gallaway M, De Land PN. Frequency of convergence insufficiency among fifth and sixth graders. The Convergence Insufficiency and Reading Study (CIRS) group. Optom Vis Sci. 1999;76:643–649. - PubMed
-
- Hokoda SC. General binocular dysfunctions in an urban optometry clinic. J Am Optom Assoc. 1985;56:560–562. - PubMed
-
- Porcar E, Martinez-Palomera A. Prevalence of general binocular dysfunctions in a population of university students. Optom Vis Sci. 1997;74:111–113. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
