

Glial fibrillary acidic protein as a brain injury biomarker in children undergoing extracorporeal membrane oxygenation
- PMID: 21057367
- PMCID: PMC3686089
- DOI: 10.1097/PCC.0b013e3181fe3ec7
Glial fibrillary acidic protein as a brain injury biomarker in children undergoing extracorporeal membrane oxygenation
Abstract
Objective: To determine whether, in children, plasma glial fibrillary acidic protein is associated with brain injury during extracorporeal membrane oxygenation and with mortality.
Design: Prospective, observational study.
Setting: Pediatric intensive care unit in an urban tertiary care academic center.
Patients: Neonatal and pediatric patients on extracorporeal membrane oxygenation (n = 22).
Interventions: Serial blood sampling for glial fibrillary acidic protein measurements.
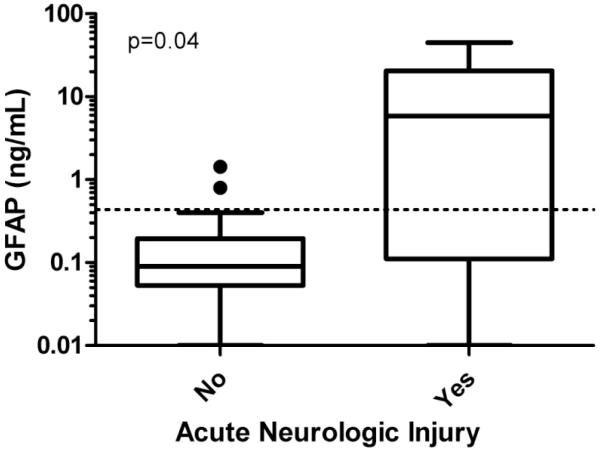
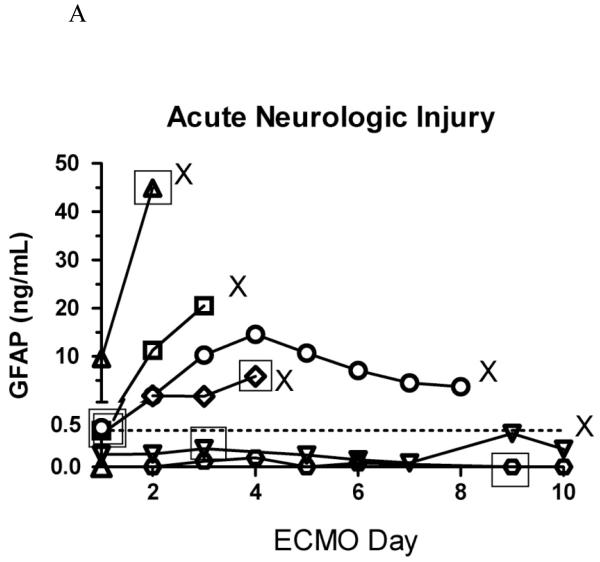
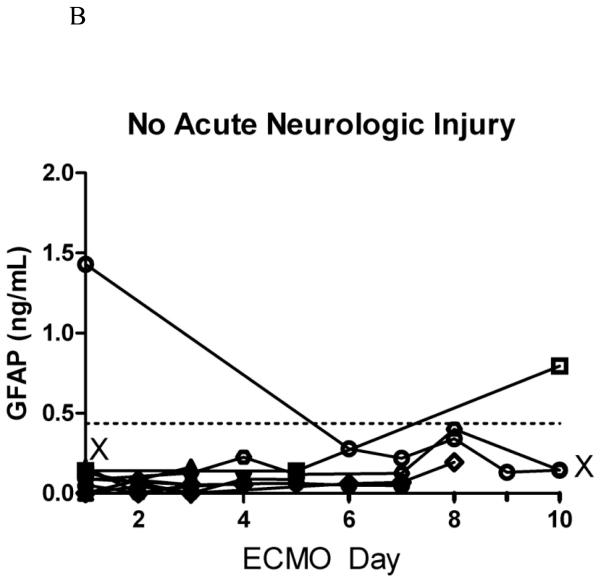
Measurements and main results: Prospective patients age 1 day to 18 yrs who required extracorporeal membrane oxygenation from April 2008 to August 2009 were studied. Glial fibrillary acidic protein was measured using an electrochemiluminescent immunoassay developed at Johns Hopkins. Control samples were collected from 99 healthy children (0.5-16 yrs) and 59 neonatal intensive care unit infants without neurologic injury. In controls, the median glial fibrillary acidic protein concentration was 0.055 ng/mL (interquartile range, 0-0.092 ng/mL) and the 95th percentile of glial fibrillary acidic protein was 0.436 ng/mL. In patients on extracorporeal membrane oxygenation, plasma glial fibrillary acidic protein was measured at 6, 12, and every 24 hrs after cannulation. We enrolled 22 children who underwent extracorporeal membrane oxygenation. Median age was 7 days (interquartile range, 2 days to 9 yrs), and primary extracorporeal membrane oxygenation indication was: cardiac failure, six of 22 (27.3%); respiratory failure, 12 of 22 (54.5%); extracorporeal cardiopulmonary resuscitation, three of 22 (13.6%); and sepsis, one of 22 (4.6%). Seven of 22 (32%) patients developed acute neurologic injury (intracranial hemorrhage, brain death, or cerebral edema diagnosed by imaging). Fifteen of 22 (68%) survived to hospital discharge. In the extracorporeal membrane oxygenation group, peak glial fibrillary acidic protein levels were higher in children with brain injury than those without (median, 5.9 vs. 0.09 ng/mL, p = .04) and in nonsurvivors compared with survivors to discharge (median, 5.9 vs. 0.09 ng/mL, p = .04). The odds ratio for brain injury for glial fibrillary acidic protein >0.436 ng/mL vs. normal was 11.5 (95% confidence interval, 1.3-98.3) and the odds ratio for mortality was 13.6 (95% confidence interval, 1.7-108.5).
Conclusions: High glial fibrillary acidic protein during extracorporeal membrane oxygenation is significantly associated with acute brain injury and death. Brain injury biomarkers may aid in outcome prediction and neurologic monitoring of patients on extracorporeal membrane oxygenation to improve outcomes and benchmark new therapies.
Figures
Comment in
-
Glial fibrillary acidic protein: a promising biomarker in pediatric brain injury.Pediatr Crit Care Med. 2011 Sep;12(5):603-4. doi: 10.1097/PCC.0b013e3182070f89. Pediatr Crit Care Med. 2011. PMID: 21897166 No abstract available.
References
-
- Conrad SA, Rycus PT, Dalton H. Extracorporeal Life Support Registry Report 2004. ASAIO J. 2005 Jan-Feb;51(1):4–10. - PubMed
-
- Morris MC, Wernovsky G, Nadkarni VM. Survival outcomes after extracorporeal cardiopulmonary resuscitation instituted during active chest compressions following refractory in-hospital pediatric cardiac arrest. Pediatr Crit Care Med. 2004 Sep;5(5):440–6. - PubMed
-
- Alsoufi B, Al-Radi OO, Nazer RI, Gruenwald C, Foreman C, Williams WG, Coles JG, Caldarone CA, Bohn DG, Van Arsdell GS. Survival outcomes after rescue extracorporeal cardiopulmonary resuscitation in pediatric patients with refractory cardiac arrest. J Thorac Cardiovasc Surg. 2007 Oct;134(4):952–959.e2. - PubMed
-
- Haines NM, Rycus PT, Zwischenberger JB, Bartlett RH, Undar A. Extracorporeal Life Support Registry Report 2008: neonatal and pediatric cardiac cases. ASAIO J. 2009 Jan-Feb;55(1):111–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K23 HL078819/HL/NHLBI NIH HHS/United States
- UL1 RR025005/RR/NCRR NIH HHS/United States
- L40 HL090401/HL/NHLBI NIH HHS/United States
- UL1 RR 025005/RR/NCRR NIH HHS/United States
- 1KL2RR025006-01/RR/NCRR NIH HHS/United States
- 5K12HL087169/HL/NHLBI NIH HHS/United States
- 5R01HL091759/HL/NHLBI NIH HHS/United States
- 5T15HL086386/HL/NHLBI NIH HHS/United States
- K12 HL087169/HL/NHLBI NIH HHS/United States
- KL2 RR025006/RR/NCRR NIH HHS/United States
- T15 HL086386/HL/NHLBI NIH HHS/United States
- R01 HL091759/HL/NHLBI NIH HHS/United States
- 1U54HL090515/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
