

Population based screening for chronic kidney disease: cost effectiveness study
- PMID: 21059726
- PMCID: PMC2975430
- DOI: 10.1136/bmj.c5869
Population based screening for chronic kidney disease: cost effectiveness study
Abstract
Objective: To determine the cost effectiveness of one-off population based screening for chronic kidney disease based on estimated glomerular filtration rate.
Design: Cost utility analysis of screening with estimated glomerular filtration rate alone compared with no screening (with allowance for incidental finding of cases of chronic kidney disease). Analyses were stratified by age, diabetes, and the presence or absence of proteinuria. Scenario and sensitivity analyses, including probabilistic sensitivity analysis, were performed. Costs were estimated in all adults and in subgroups defined by age, diabetes, and hypertension.
Setting: Publicly funded Canadian healthcare system.
Participants: Large population based laboratory cohort used to estimate mortality rates and incidence of end stage renal disease for patients with chronic kidney disease over a five year follow-up period. Patients had not previously undergone assessment of glomerular filtration rate.
Main outcome measures: Lifetime costs, end stage renal disease, quality adjusted life years (QALYs) gained, and incremental cost per QALY gained.
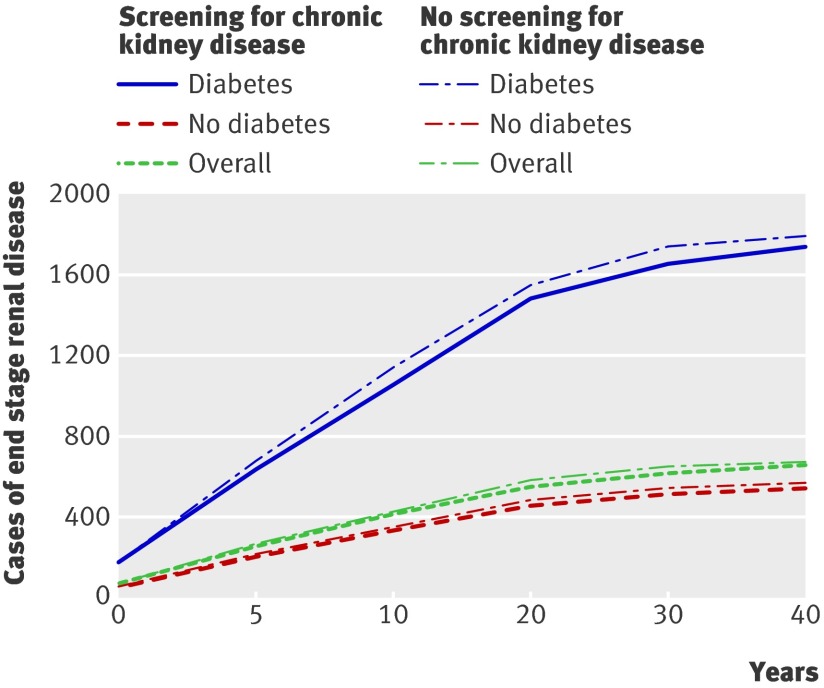
Results: Compared with no screening, population based screening for chronic kidney disease was associated with an incremental cost of $C463 (Canadian dollars in 2009; equivalent to about £275, €308, US $382) and a gain of 0.0044 QALYs per patient overall, representing a cost per QALY gained of $C104 900. In a cohort of 100 000 people, screening for chronic kidney disease would be expected to reduce the number of people who develop end stage renal disease over their lifetime from 675 to 657. In subgroups of people with and without diabetes, the cost per QALY gained was $C22 600 and $C572 000, respectively. In a cohort of 100 000 people with diabetes, screening would be expected to reduce the number of people who develop end stage renal disease over their lifetime from 1796 to 1741. In people without diabetes with and without hypertension, the cost per QALY gained was $C334 000 and $C1 411 100, respectively.
Conclusions: Population based screening for chronic kidney disease with assessment of estimated glomerular filtration rate is not cost effective overall or in subgroups of people with hypertension or older people. Targeted screening of people with diabetes is associated with a cost per QALY that is similar to that accepted in other interventions funded by public healthcare systems.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures


Comment in
-
Screening for chronic kidney disease.BMJ. 2010 Nov 8;341:c5734. doi: 10.1136/bmj.c5734. BMJ. 2010. PMID: 21059725 No abstract available.
References
-
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39(suppl 1):1-266s. - PubMed
-
- McClellan WM, Ramirez SP, Jurkovitz C. Screening for chronic kidney disease: unresolved issues. J Am Soc Nephrol 2003;14(suppl 2):81-7s. - PubMed
-
- Brown WW, Collins A, Chen SC, King K, Molony D, Gannon MR, et al. Identification of persons at high risk for kidney disease via targeted screening: the NKF Kidney Early Evaluation Program. Kidney Int Suppl 2003;83:50-5s. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical