

Low-dose hydrocortisone in patients with cirrhosis and septic shock: a randomized controlled trial
- PMID: 21059778
- PMCID: PMC3001503
- DOI: 10.1503/cmaj.090707
Low-dose hydrocortisone in patients with cirrhosis and septic shock: a randomized controlled trial
Abstract
Background: Recent studies have reported a high prevalence of relative adrenal insufficiency in patients with liver cirrhosis. However, the effect of corticosteroid replacement on mortality in this high-risk group remains unclear. We examined the effect of low-dose hydrocortisone in patients with cirrhosis who presented with septic shock.
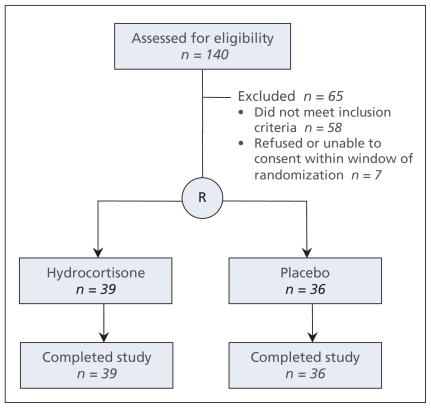
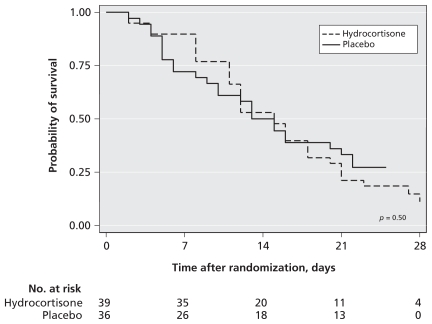
Methods: We enrolled patients with cirrhosis and septic shock aged 18 years or older in a randomized double-blind placebo-controlled trial. Relative adrenal insufficiency was defined as a serum cortisol increase of less than 250 nmol/L or 9 μg/dL from baseline after stimulation with 250 μg of intravenous corticotropin. Patients were assigned to receive 50 mg of intravenous hydrocortisone or placebo every six hours until hemodynamic stability was achieved, followed by steroid tapering over eight days. The primary outcome was 28-day all-cause mortality.
Results: The trial was stopped for futility at interim analysis after 75 patients were enrolled. Relative adrenal insufficiency was diagnosed in 76% of patients. Compared with the placebo group (n = 36), patients in the hydrocortisone group (n = 39) had a significant reduction in vasopressor doses and higher rates of shock reversal (relative risk [RR] 1.58, 95% confidence interval [CI] 0.98-2.55, p = 0.05). Hydrocortisone use was not associated with a reduction in 28-day mortality (RR 1.17, 95% CI 0.92-1.49, p = 0.19) but was associated with an increase in shock relapse (RR 2.58, 95% CI 1.04-6.45, p = 0.03) and gastrointestinal bleeding (RR 3.00, 95% CI 1.08-8.36, p = 0.02).
Interpretation: Relative adrenal insufficiency was very common in patients with cirrhosis presenting with septic shock. Despite initial favourable effects on hemodynamic parameters, hydrocortisone therapy did not reduce mortality and was associated with an increase in adverse effects. (Current Controlled Trials registry no. ISRCTN99675218.).
Figures
References
-
- Hoyert DL, Kung HC, Smith BL. Deaths: preliminary data for 2003. Natl Vital Stat Rep 2005;53:1–48 - PubMed
-
- Vashist Y, Semela D, Dufour JF. Hyperdynamic circulation in liver cirrhosis: desensitization of vasoconstrictive receptors by G protein-coupled receptor kinases. Med Hypotheses 2004;62:82–5 - PubMed
-
- Newby DE, Hayes PC. Hyperdynamic circulation in liver cirrhosis: not peripheral vasodilatation but ‘splanchnic steal’.QJM 2002;95:827–30 - PubMed
-
- Arkenau HT, Stichtenoth DO, Frolich JC, et al. Elevated nitric oxide levels in patients with chronic liver disease and cirrhosis correlate with disease stage and parameters of hyperdynamic circulation. Z Gastroenterol 2002;40:907–13 - PubMed
-
- Gaenzer H, Sturm W, Neumayr G, et al. Hyperdynamic circulation in liver cirrhosis: no evidence for peripheral vasodilation detected by ultrasound of the brachial artery. Am J Gastroenterol 2000;95:551–2 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical