

Impact of the human circadian system, exercise, and their interaction on cardiovascular function
- PMID: 21059915
- PMCID: PMC2996667
- DOI: 10.1073/pnas.1006749107
Impact of the human circadian system, exercise, and their interaction on cardiovascular function
Abstract
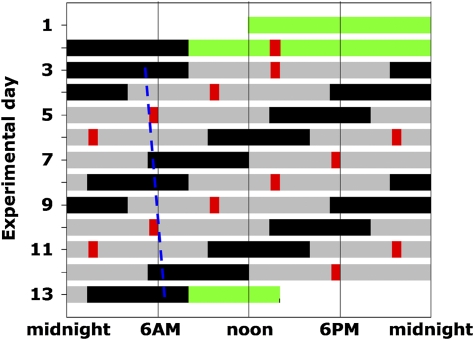
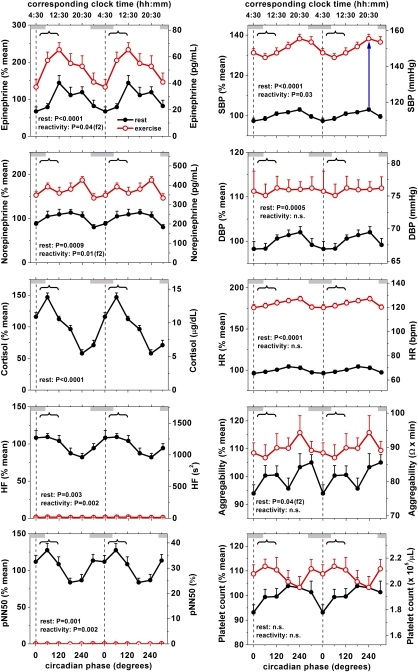
The risk of adverse cardiovascular events peaks in the morning (≈9:00 AM) with a secondary peak in the evening (≈8:00 PM) and a trough at night. This pattern is generally believed to be caused by the day/night distribution of behavioral triggers, but it is unknown whether the endogenous circadian system contributes to these daily fluctuations. Thus, we tested the hypotheses that the circadian system modulates autonomic, hemodynamic, and hemostatic risk markers at rest, and that behavioral stressors have different effects when they occur at different internal circadian phases. Twelve healthy adults were each studied in a 240-h forced desynchrony protocol in dim light while standardized rest and exercise periods were uniformly distributed across the circadian cycle. At rest, there were large circadian variations in plasma cortisol (peak-to-trough ≈85% of mean, peaking at a circadian phase corresponding to ≈9:00 AM) and in circulating catecholamines (epinephrine, ≈70%; norepinephrine, ≈35%, peaking during the biological day). At ≈8:00 PM, there was a circadian peak in blood pressure and a trough in cardiac vagal modulation. Sympathetic variables were consistently lowest and vagal markers highest during the biological night. We detected no simple circadian effect on hemostasis, although platelet aggregability had two peaks: at ≈noon and ≈11:00 PM. There was circadian modulation of the cardiovascular reactivity to exercise, with greatest vagal withdrawal at ≈9:00 AM and peaks in catecholamine reactivity at ≈9:00 AM and ≈9:00 PM. Thus, the circadian system modulates numerous cardiovascular risk markers at rest as well as their reactivity to exercise, with resultant profiles that could potentially contribute to the day/night pattern of adverse cardiovascular events.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Lloyd-Jones D, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2009 update: A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119:e21–e181. - PubMed
-
- Allender S, et al. European Cardiovascular Disease Statistics 2008. British Heart Foundation and University of Oxford, Oxford; 2008.
-
- Muller JE, et al. Circadian variation in the frequency of onset of acute myocardial infarction. N Engl J Med. 1985;313:1315–1322. - PubMed
-
- Ridker PM, Manson JE, Buring JE, Muller JE, Hennekens CH. Circadian variation of acute myocardial infarction and the effect of low-dose aspirin in a randomized trial of physicians. Circulation. 1990;82:897–902. - PubMed
-
- Cannon CP, et al. Circadian variation in the onset of unstable angina and non-Q-wave acute myocardial infarction (the TIMI III Registry and TIMI IIIB) Am J Cardiol. 1997;79:253–258. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K24 HL076446/HL/NHLBI NIH HHS/United States
- M01-RR02635/RR/NCRR NIH HHS/United States
- K99-HL102241/HL/NHLBI NIH HHS/United States
- K99 HL102241/HL/NHLBI NIH HHS/United States
- M01 RR002635/RR/NCRR NIH HHS/United States
- P30 HL101299/HL/NHLBI NIH HHS/United States
- K24-HL093218/HL/NHLBI NIH HHS/United States
- R01-HL76409/HL/NHLBI NIH HHS/United States
- K24-HL076446/HL/NHLBI NIH HHS/United States
- K24 HL093218/HL/NHLBI NIH HHS/United States
- P30-HL101299/HL/NHLBI NIH HHS/United States
- R01 HL076409/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
