

The Disablement in the Physically Active Scale, part II: the psychometric properties of an outcomes scale for musculoskeletal injuries
- PMID: 21062187
- PMCID: PMC2978015
- DOI: 10.4085/1062-6050-45.6.630
The Disablement in the Physically Active Scale, part II: the psychometric properties of an outcomes scale for musculoskeletal injuries
Abstract
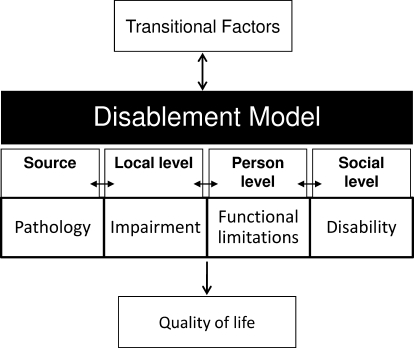
Context: Outcomes assessment is an integral part of ensuring quality in athletic training, but few generic instruments have been specifically designed to measure disablement in the physically active.
Objective: To assess the psychometric properties of the Disablement in the Physically Active Scale (DPA), a patient-report, generic outcomes instrument.
Design: Observational study.
Setting: We collected data in 5 settings with competitive and recreational athletes. Participants entered into the study at 3 distinct points: (1) when healthy and (2) after an acute injury, or (3) after a persistent injury.
Patients or other participants: Measures were obtained from 368 baseline participants (202 females, 166 males; age = 20.1 ± 3.8 years), 54 persistent participants (32 females, 22 males; age = 22.0 ± 8.3 years), and 28 acutely injured participants (8 females, 20 males; age = 19.8 ± 1.90 years).
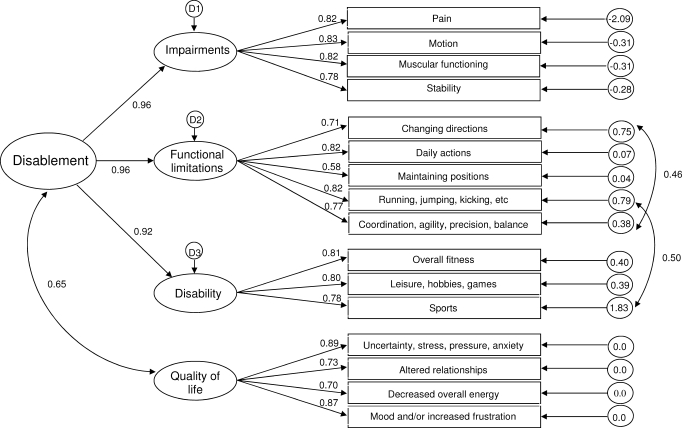
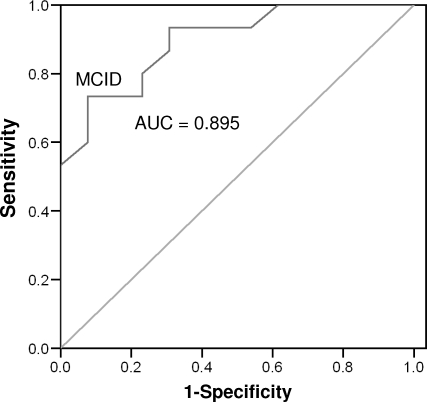
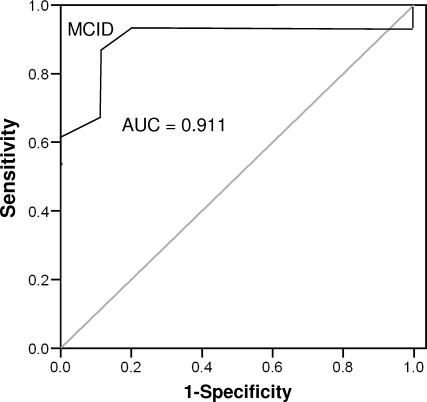
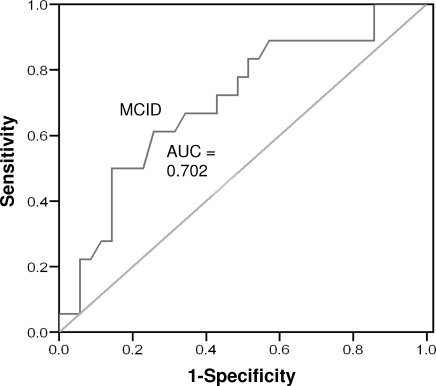
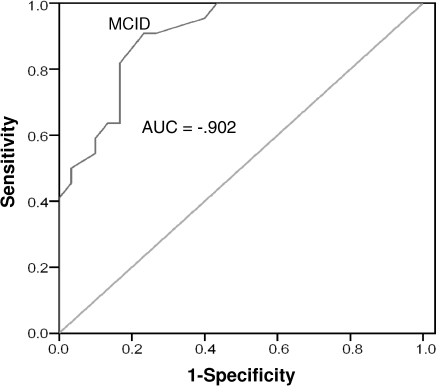
Main outcome measure(s): We assessed internal consistency with a Cronbach α and test-retest reliability with intraclass correlation (2,1) values. The scale's factor structure was assessed with a hierarchical confirmatory factor analysis. Concurrent validity was assessed with a Pearson correlation. Responsiveness was calculated using a receiver operating characteristic curve and a minimal clinically important difference value.
Results: The Cronbach α scores for the DPA were 0.908 and 0.890 in acute and persistent groups, respectively. The intraclass correlation (2,1) value of the DPA was 0.943 (95% confidence interval = 0.885, 0.972). The fit indices values were 1.89, 0.852, 0.924, 0.937, and 0.085 (90% confidence interval = 0.066, 0.103) for the minimum sample discrepancy divided by degrees of freedom, goodness-of-fit index, Tucker-Lewis Index, comparative fit index, and root mean square error of approximation, respectively. The DPA scores accounted for 51% to 56.4% of the variation in global functioning scores. The area under the curve was statistically significant, and the minimally clinically important difference values were established.
Conclusions: The DPA is a reliable, valid, and responsive instrument.
Figures
References
-
- Donabedian A. The Criteria and Standards of Quality. Vol 2. Ann Arbor, MI: Health Administration Press; 1982. pp. 1–13.
-
- Donabedian A. Quality assessment and assurance: unity of purpose, diversity of means. Inquiry. 1998;25(1):173–192. - PubMed
-
- Donabedian A. An Introduction to Quality Assurance in Health Care. New York, NY: Oxford University Press; 2003. pp. 45–56.
-
- Sackett D. L., Straus S. E., Richardson W. J., Rosenberg W., Haynes R. B. Evidence-Based Medicine: How to Practice and Teach EBM. Vol 2. Edinburgh, Scotland: Churchill Livingstone; 2000.
-
- Lowenstein R. The quality cure? The New York Times Magazine. March 13, 2005;6:46–51.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
