

Differences in organ dysfunctions between neonates and older children: a prospective, observational, multicenter study
- PMID: 21062434
- PMCID: PMC3219976
- DOI: 10.1186/cc9323
Differences in organ dysfunctions between neonates and older children: a prospective, observational, multicenter study
Abstract
Introduction: The multiple organ dysfunction syndrome (MODS) is a major cause of death for patients admitted to pediatric intensive care units (PICU). The Pediatric Logistic Organ Dysfunction (PELOD) score has been validated in order to describe and quantify the severity of organ dysfunction (OD). There are several physiological differences between neonates and older children. The objective of the study was to determine whether there are differences in incidence of ODs and mortality rate between full-term neonates (age <28 days) and older children.
Methods: In a prospective, observational study, 1806 patients, admitted to seven PICUs between September 1998 and February 2000 were included. The PELOD score, which includes six organ dysfunctions and 12 variables, was recorded daily. For each variable, the most abnormal value was used to define the daily OD. For each OD, the most abnormal value each day and that during the entire stay were used in calculating the daily PELOD and PELOD scores, respectively. The relationships between OD, daily OD, PELOD, daily PELOD and mortality were compared between the two strata (neonates, older children) based on the discrimination power, logistic and multiple regression analyses.
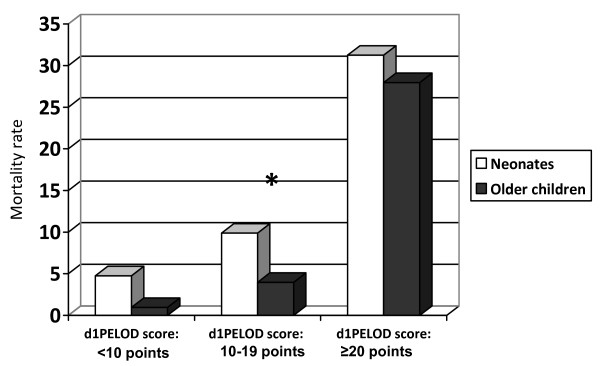
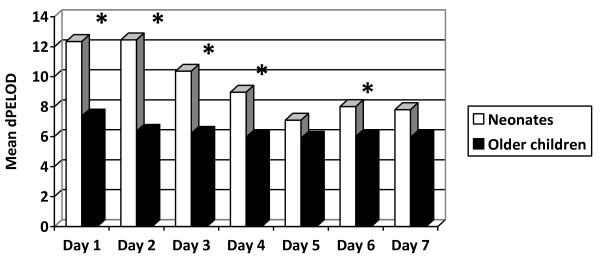
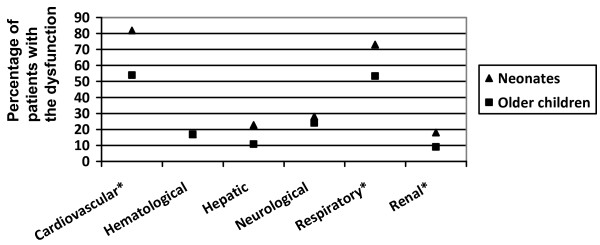
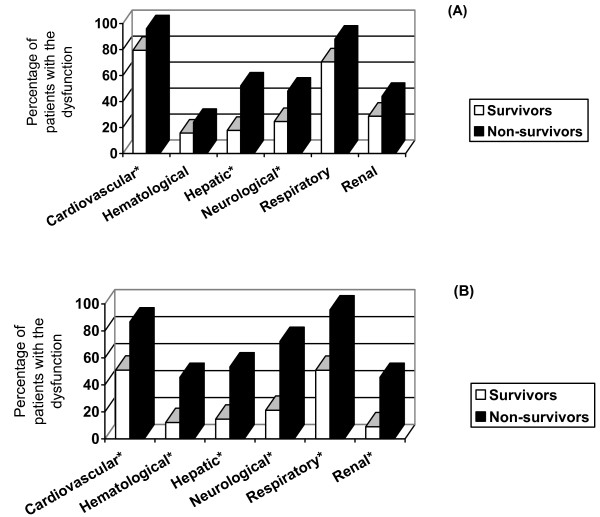
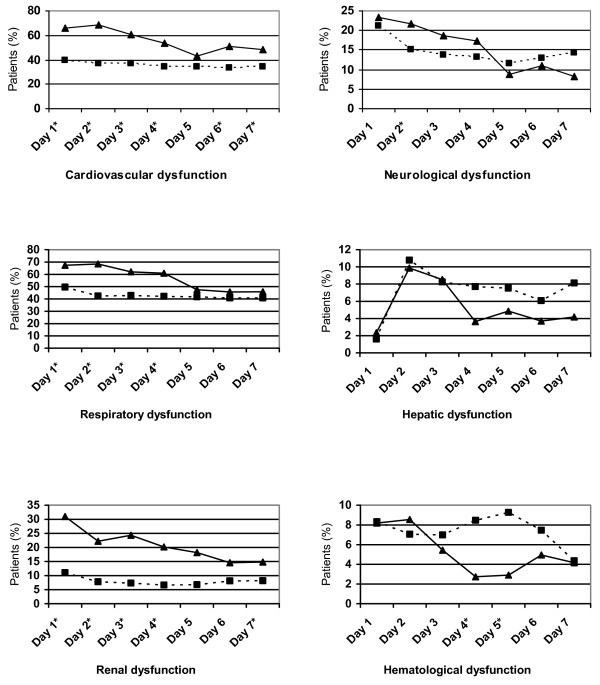
Results: Of the 1806 enrolled patients 171 (9.5%) were neonates. Incidence of MODS and mortality rate were higher among neonates than in older children (14.6% vs. 5.5%, P < 10(-7); 75.4%, vs. 50.9%, P < 10(-4); respectively). Daily PELOD scores were significantly higher in neonates from day 1 to day 4. Daily cardiovascular, respiratory and renal dysfunction scores from day 1 to day 4 as well as the PELOD score for the entire pediatric intensive care unit stay were also significantly higher in neonates. Neurological, cardiovascular, and hepatic dysfunctions were independent predictors of death among neonates while all ODs significantly contributed to the risk of mortality in older children.
Conclusions: Our data demonstrate that incidence of MODS and mortality rate are higher among neonates compared to older children. Neurological, cardiovascular, and hepatic dysfunctions were the only significant contributors to neonatal mortality. Stratification for neonates versus older children might be useful in clinical trials where MODS is considered as an outcome measure.
Figures
References
-
- Graciano AL, Balko JA, Rahn DS, Ahmad N, Giroir BP. The Pediatric Multiple Organ Dysfunction Score (P-MODS): development and validation of an objective scale to measure the severity of multiple organ dysfunction in critically ill children. Crit Care Med. 2005;33:1484–1491. doi: 10.1097/01.CCM.0000170943.23633.47. - DOI - PubMed
-
- Leteurtre S, Martinot A, Duhamel A, Proulx F, Grandbastien B, Cotting J, Gottesman R, Joffe A, Pfenninger J, Hubert P, Lacroix J, Leclerc F. Validation of the paediatric logistic organ dysfunction (PELOD) score: prospective, observational, multicentre study. Lancet. 2003;362:192–197. doi: 10.1016/S0140-6736(03)13908-6. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
