

Automated left ventricular diastolic function evaluation from phase-contrast cardiovascular magnetic resonance and comparison with Doppler echocardiography
- PMID: 21062448
- PMCID: PMC2991299
- DOI: 10.1186/1532-429X-12-63
Automated left ventricular diastolic function evaluation from phase-contrast cardiovascular magnetic resonance and comparison with Doppler echocardiography
Abstract
Background: Early detection of diastolic dysfunction is crucial for patients with incipient heart failure. Although this evaluation could be performed from phase-contrast (PC) cardiovascular magnetic resonance (CMR) data, its usefulness in clinical routine is not yet established, mainly because the interpretation of such data remains mostly based on manual post-processing. Accordingly, our goal was to develop a robust process to automatically estimate velocity and flow rate-related diastolic parameters from PC-CMR data and to test the consistency of these parameters against echocardiography as well as their ability to characterize left ventricular (LV) diastolic dysfunction.
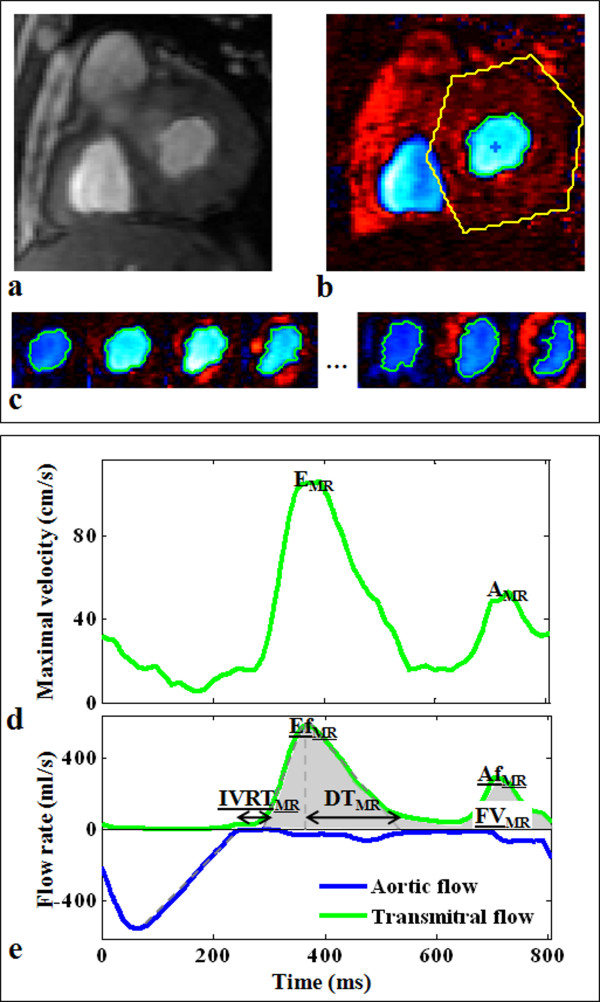
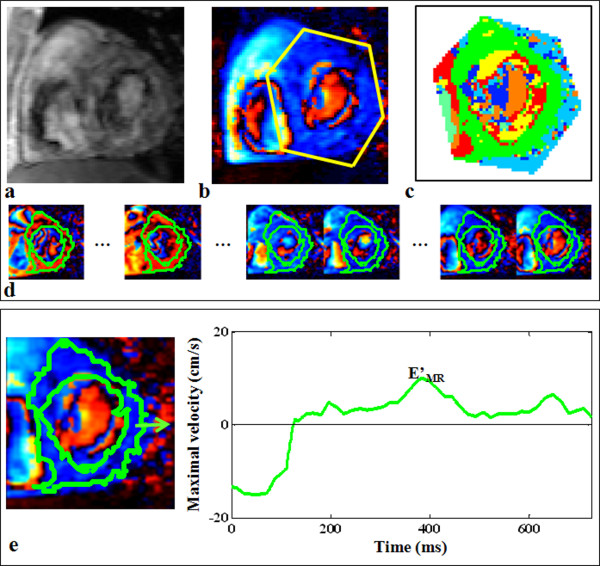
Results: We studied 35 controls and 18 patients with severe aortic valve stenosis and preserved LV ejection fraction who had PC-CMR and Doppler echocardiography exams on the same day. PC-CMR mitral flow and myocardial velocity data were analyzed using custom software for semi-automated extraction of diastolic parameters. Inter-operator reproducibility of flow pattern segmentation and functional parameters was assessed on a sub-group of 30 subjects. The mean percentage of overlap between the transmitral flow segmentations performed by two independent operators was 99.7 ± 1.6%, resulting in a small variability (<1.96 ± 2.95%) in functional parameter measurement. For maximal myocardial longitudinal velocities, the inter-operator variability was 4.25 ± 5.89%. The MR diastolic parameters varied significantly in patients as opposed to controls (p < 0.0002). Both velocity and flow rate diastolic parameters were consistent with echocardiographic values (r > 0.71) and receiver operating characteristic (ROC) analysis revealed their ability to separate patients from controls, with sensitivity > 0.80, specificity > 0.80 and accuracy > 0.85. Slight superiority in terms of correlation with echocardiography (r = 0.81) and accuracy to detect LV abnormalities (sensitivity > 0.83, specificity > 0.91 and accuracy > 0.89) was found for the PC-CMR flow-rate related parameters.
Conclusions: A fast and reproducible technique for flow and myocardial PC-CMR data analysis was successfully used on controls and patients to extract consistent velocity-related diastolic parameters, as well as flow rate-related parameters. This technique provides a valuable addition to established CMR tools in the evaluation and the management of patients with diastolic dysfunction.
Figures



References
-
- Persson H, Lonn E, Edner M, Baruch L, Lang CC, Morton JJ, Ostergren J, McKelvie RS. Diastolic dysfunction in heart failure with preserved systolic function: need for objective evidence:results from the CHARM Echocardiographic Substudy-CHARMES. J Am Coll Cardiol. 2007;49:687–694. doi: 10.1016/j.jacc.2006.08.062. - DOI - PubMed
-
- Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA, Waggoner AD, Flachskampf FA, Pellikka PA, Evangelista A. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr. 2009;22:107–133. doi: 10.1016/j.echo.2008.11.023. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
