

Does intensive insulin therapy really reduce mortality in critically ill surgical patients? A reanalysis of meta-analytic data
- PMID: 21062514
- PMCID: PMC3219247
- DOI: 10.1186/cc9240
Does intensive insulin therapy really reduce mortality in critically ill surgical patients? A reanalysis of meta-analytic data
Abstract
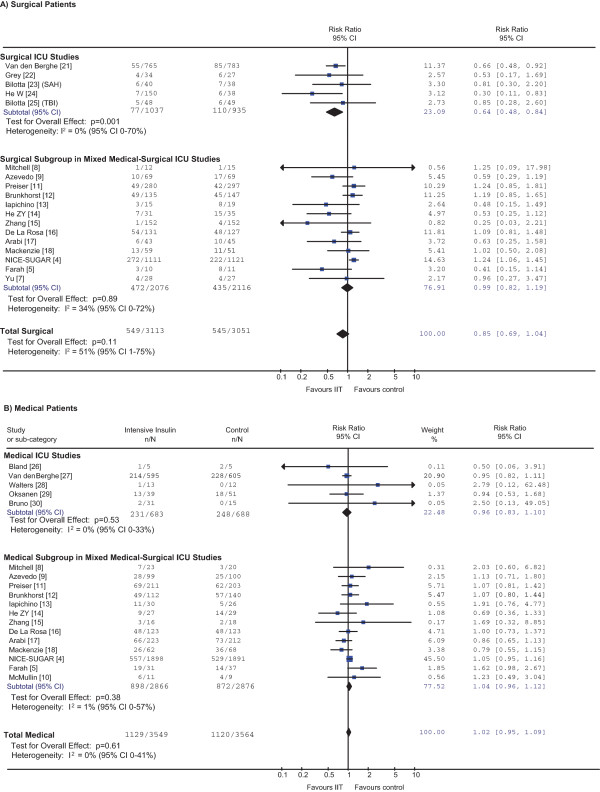
Two recent systematic reviews evaluating intensive insulin therapy (IIT) in critically ill patients grouped randomized controlled trials (RCTs) by type of intensive care unit (ICU). The more recent review found that IIT reduced mortality in patients admitted to a surgical ICU, but not in those admitted to medical ICUs or mixed medical-surgical ICUs, or in all patients combined. Our objective was to determine whether IIT saves lives in critically ill surgical patients regardless of the type of ICU. Pooling mortality data from surgical and medical subgroups in mixed-ICU RCTs (16 trials) with RCTs conducted exclusively in surgical ICUs (five trials) and in medical ICUs (five trials), respectively, showed no effect of IIT in the subgroups of surgical patients (risk ratio = 0.85, 95% confidence interval (CI) = 0.69 to 1.04, P = 0.11; I2 = 51%, 95% CI = 1 to 75%) or of medical patients (risk ratio = 1.02, 95% CI = 0.95 to 1.09, P = 0.61; I2 = 0%, 95% CI = 0 to 41%). There was no differential effect between subgroups (interaction P = 0.10). There was statistical heterogeneity in the surgical subgroup, with some trials demonstrating significant benefit and others demonstrating significant harm, but no surgical subgroup consistently benefited from IIT. Such a reanalysis suggests that IIT does not reduce mortality in critically ill surgical patients or medical patients. Further insights may come from individual patient data meta-analyses or from future large multicenter RCTs in more narrowly defined subgroups of surgical patients.
Figures
References
-
- Griesdale DEG, de Souza RJ, van Dam RM, Heyland DK, Cook DJ, Malhotra A, Dhaliwal R, Henderson WR, Chittock DR, Finder S, Talmor D. Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE-SUGAR study data. CMAJ. 2009;180:821–827. doi: 10.1503/cmaj.090206. - DOI - PMC - PubMed
-
- Farah R, Samokhvalov A, Zviebel F, Makhoul N. Insulin therapy of hyperglycemia in intensive care. Isr Med Assoc J. 2007;9:140–142. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
