

Circulating angiogenic and antiangiogenic factors in women with eclampsia
- PMID: 21062661
- PMCID: PMC3057127
- DOI: 10.1016/j.ajog.2010.08.049
Circulating angiogenic and antiangiogenic factors in women with eclampsia
Abstract
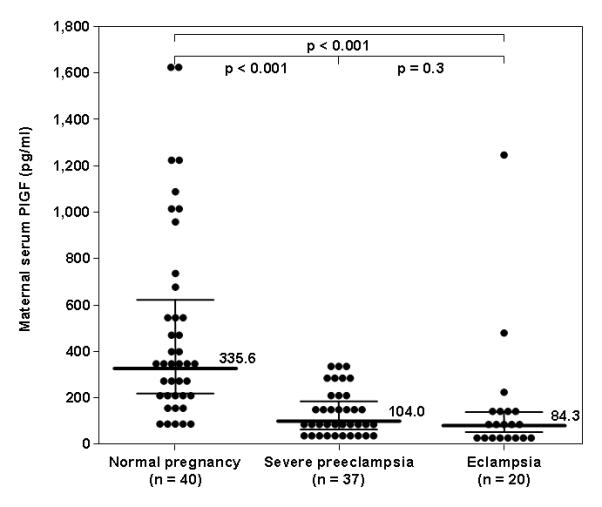
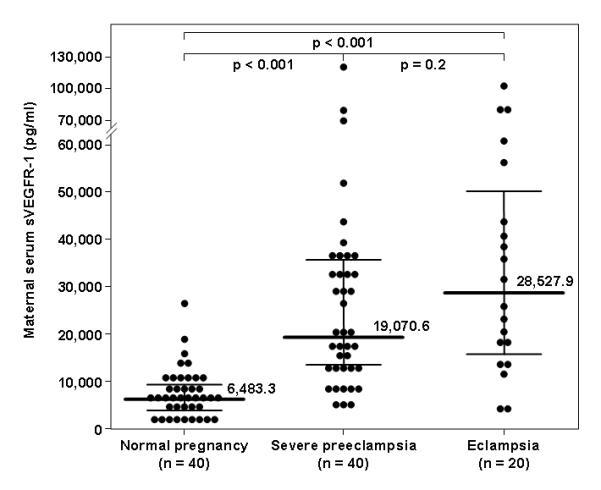
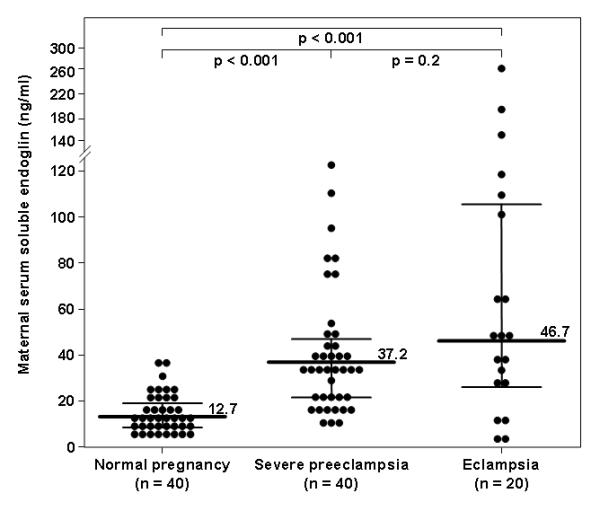
Objective: The objective of the study was to determine whether eclampsia has a different circulating profile of angiogenic (placental growth factor [PlGF]) and antiangiogenic factors (soluble vascular endothelial growth factor receptor-1 [sVEGFR-1] and soluble endoglin [sEng]) from severe preeclampsia.
Study design: This cross-sectional study included pregnant women in the following groups: (1) normal pregnancy (n = 40); (2) severe preeclampsia (n = 40); and (3) eclampsia (n = 20). Maternal serum PlGF, sVEGFR-1, and sEng concentrations were determined using an enzyme-linked immunosorbent assay.
Results: The study results included the following: (1) the median concentration of sVEGFR-1 and sEng was higher and of PlGF was lower in severe preeclampsia or eclampsia than in normal pregnancy (P < .001 for all); and (2) the median concentrations of these 3 analytes did not differ significantly between patients with severe preeclampsia and those with eclampsia.
Conclusion: Eclampsia is associated with higher maternal circulating concentrations of sVEGFR-1 and sEng and lower concentrations of PlGF than normal pregnancy but with similar concentrations to severe preeclampsia. These findings suggest that eclampsia shares a common pathogenic pathway as severe preeclampsia.
Published by Mosby, Inc.
Figures
Similar articles
-
Maternal plasma concentrations of angiogenic/antiangiogenic factors in the third trimester of pregnancy to identify the patient at risk for stillbirth at or near term and severe late preeclampsia.Am J Obstet Gynecol. 2013 Apr;208(4):287.e1-287.e15. doi: 10.1016/j.ajog.2013.01.016. Epub 2013 Jan 17. Am J Obstet Gynecol. 2013. PMID: 23333542 Free PMC article.
-
Late-onset preeclampsia is associated with an imbalance of angiogenic and anti-angiogenic factors in patients with and without placental lesions consistent with maternal underperfusion.J Matern Fetal Neonatal Med. 2012 May;25(5):498-507. doi: 10.3109/14767058.2011.591461. Epub 2011 Aug 25. J Matern Fetal Neonatal Med. 2012. PMID: 21867402 Free PMC article.
-
A prospective cohort study of the value of maternal plasma concentrations of angiogenic and anti-angiogenic factors in early pregnancy and midtrimester in the identification of patients destined to develop preeclampsia.J Matern Fetal Neonatal Med. 2009 Nov;22(11):1021-38. doi: 10.3109/14767050902994754. J Matern Fetal Neonatal Med. 2009. PMID: 19900040 Free PMC article.
-
Accuracy of circulating placental growth factor, vascular endothelial growth factor, soluble fms-like tyrosine kinase 1 and soluble endoglin in the prediction of pre-eclampsia: a systematic review and meta-analysis.BJOG. 2012 Jun;119(7):778-87. doi: 10.1111/j.1471-0528.2012.03311.x. Epub 2012 Mar 20. BJOG. 2012. PMID: 22433027
-
Angiogenic factors and preeclampsia.Front Biosci. 2007 Jan 1;12:2395-402. doi: 10.2741/2241. Front Biosci. 2007. PMID: 17127249 Review.
Cited by
-
Placental C4d deposition is a feature of defective placentation: observations in cases of preeclampsia and miscarriage.Virchows Arch. 2015 Jun;466(6):717-25. doi: 10.1007/s00428-015-1759-y. Epub 2015 Mar 28. Virchows Arch. 2015. PMID: 25820373
-
Placental Growth Factor as a Prognostic Tool in Women With Hypertensive Disorders of Pregnancy: A Systematic Review.Hypertension. 2017 Dec;70(6):1228-1237. doi: 10.1161/HYPERTENSIONAHA.117.10150. Epub 2017 Oct 30. Hypertension. 2017. PMID: 29084878 Free PMC article.
-
Is an episode of suspected preterm labor that subsequently leads to a term delivery benign?Am J Obstet Gynecol. 2017 Feb;216(2):89-94. doi: 10.1016/j.ajog.2016.12.030. Am J Obstet Gynecol. 2017. PMID: 28148450 Free PMC article. No abstract available.
-
Vascular Endothelial Growth Factor and Podocyte Protection in Chronic Hypoxia: Effects of Endothelin-A Receptor Antagonism.Am J Nephrol. 2016;43(2):74-84. doi: 10.1159/000444719. Epub 2016 Mar 2. Am J Nephrol. 2016. PMID: 26930122 Free PMC article.
-
The Impact of Magnesium Sulfate Therapy on Angiogenic Factors in Preeclampsia.Pregnancy Hypertens. 2012 Jan 1;2(1):16-21. doi: 10.1016/j.preghy.2011.08.118. Pregnancy Hypertens. 2012. PMID: 22247820 Free PMC article.
References
-
- Romero R. Prenatal medicine: the child is the father of the man. 1996. J Matern.Fetal Neonatal Med. 2009;22:636–39. - PubMed
-
- Di Renzo GC. The great obstetrical syndromes. J Matern.Fetal Neonatal Med. 2009;22:633–35. - PubMed
-
- Sibai B, Dekker G, Kupferminc M. Pre-eclampsia. Lancet. 2005;365:785–99. - PubMed
-
- Friedman SA, Schiff E, Kao L, Sibai BM. Neonatal outcome after preterm delivery for preeclampsia. Am J Obstet Gynecol. 1995;172:1785–88. - PubMed
-
- MacKay AP, Berg CJ, Atrash HK. Pregnancy-related mortality from preeclampsia and eclampsia. Obstet.Gynecol. 2001;97:533–38. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
