

Endobronchial intubation detected by insertion depth of endotracheal tube, bilateral auscultation, or observation of chest movements: randomised trial
- PMID: 21062875
- PMCID: PMC2977961
- DOI: 10.1136/bmj.c5943
Endobronchial intubation detected by insertion depth of endotracheal tube, bilateral auscultation, or observation of chest movements: randomised trial
Abstract
Objective: To determine which bedside method of detecting inadvertent endobronchial intubation in adults has the highest sensitivity and specificity.
Design: Prospective randomised blinded study.
Setting: Department of anaesthesia in tertiary academic hospital.
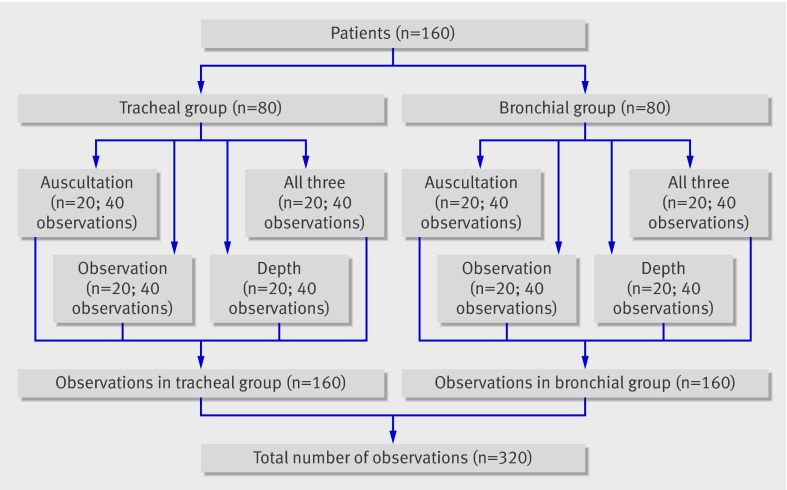
Participants: 160 consecutive patients (American Society of Anesthesiologists category I or II) aged 19-75 scheduled for elective gynaecological or urological surgery.
Interventions: Patients were randomly assigned to eight study groups. In four groups, an endotracheal tube was fibreoptically positioned 2.5-4.0 cm above the carina, whereas in the other four groups the tube was positioned in the right mainstem bronchus. The four groups differed in the bedside test used to verify the position of the endotracheal tube. To determine whether the tube was properly positioned in the trachea, in each patient first year residents and experienced anaesthetists were randomly assigned to independently perform bilateral auscultation of the chest (auscultation); observation and palpation of symmetrical chest movements (observation); estimation of the position of the tube by the insertion depth (tube depth); or a combination of all three (all three).
Main outcome measures: Correct and incorrect judgments of endotracheal tube position.
Results: 160 patients underwent 320 observations by experienced and inexperienced anaesthetists. First year residents missed endobronchial intubation by auscultation in 55% of cases and performed significantly worse than experienced anaesthetists with this bedside test (odds ratio 10.0, 95% confidence interval 1.4 to 434). With a sensitivity of 88% (95% confidence interval 75% to 100%) and 100%, respectively, tube depth and the three tests combined were significantly more sensitive for detecting endobronchial intubation than auscultation (65%, 49% to 81%) or observation(43%, 25% to 60%) (P<0.001). The four tested methods had the same specificity for ruling out endobronchial intubation (that is, confirming correct tracheal intubation). The average correct tube insertion depth was 21 cm in women and 23 cm in men. By inserting the tube to these distances, however, the distal tip of the tube was less than 2.5 cm away from the carina (the recommended safety distance, to prevent inadvertent endobronchial intubation with changes in the position of the head in intubated patients) in 20% (24/118) of women and 18% (7/42) of men. Therefore optimal tube insertion depth was considered to be 20 cm in women and 22 cm in men.
Conclusion: Less experienced clinicians should rely more on tube insertion depth than on auscultation to detect inadvertent endobronchial intubation. But even experienced physicians will benefit from inserting tubes to 20-21 cm in women and 22-23 cm in men, especially when high ambient noise precludes accurate auscultation (such as in emergency situations or helicopter transport). The highest sensitivity and specificity for ruling out endobronchial intubation, however, is achieved by combining tube depth, auscultation of the lungs, and observation of symmetrical chest movements.
Trial registration: NCT01232166.
Conflict of interest statement
Contributors: CS, PK, and SCK contributed to the design of the trial. CS, PK, SCK, and DIS contributed to the interpretation of the results and writing of the manuscript. AL, AS, CG, SCK, CW, and CS contributed to the recruitment of patients, data collection, and management of the trial. CS, DIS, and HH contributed to the statistical analysis. CS is the guarantor.
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Avoidance of endobronchial intubation.BMJ. 2010 Nov 9;341:c5936. doi: 10.1136/bmj.c5936. BMJ. 2010. PMID: 21062874 No abstract available.
Similar articles
-
Use of the Rapiscope vs chest auscultation for detection of accidental bronchial intubation in non-obese patients undergoing laparoscopic cholecystectomy.J Clin Anesth. 2006 Mar;18(2):118-23. doi: 10.1016/j.jclinane.2005.08.008. J Clin Anesth. 2006. PMID: 16563329 Clinical Trial.
-
Does the Murphy eye reduce the reliability of chest auscultation in detecting endobronchial intubation?Anesth Analg. 1999 Jun;88(6):1380-3. doi: 10.1097/00000539-199906000-00033. Anesth Analg. 1999. PMID: 10357348 Clinical Trial.
-
Cuff depth and continuous chest auscultation method for determination of tracheal tube insertion depth in nasal intubation: observational study.J Anesth. 2016 Apr;30(2):193-8. doi: 10.1007/s00540-015-2110-0. Epub 2015 Nov 30. J Anesth. 2016. PMID: 26620185
-
Tracheal tube-tip displacement in children during head-neck movement--a radiological assessment.Br J Anaesth. 2006 Apr;96(4):486-91. doi: 10.1093/bja/ael014. Epub 2006 Feb 7. Br J Anaesth. 2006. PMID: 16464981 Review.
-
Verification of endotracheal tube position.Anesthesiol Clin North Am. 2001 Dec;19(4):813-39. doi: 10.1016/s0889-8537(01)80012-2. Anesthesiol Clin North Am. 2001. PMID: 11778382 Review.
Cited by
-
Realtime and noninvasive assessment of endotracheal tube displacement using near-infrared and visible cameras.Biomed Opt Express. 2024 Oct 14;15(11):6355-6369. doi: 10.1364/BOE.531815. eCollection 2024 Nov 1. Biomed Opt Express. 2024. PMID: 39553880 Free PMC article.
-
Role of upper airway ultrasound in airway management.J Intensive Care. 2016 Aug 15;4:52. doi: 10.1186/s40560-016-0174-z. eCollection 2016. J Intensive Care. 2016. PMID: 27529028 Free PMC article. Review.
-
Detecting Endotracheal Tube and Carina on Portable Supine Chest Radiographs Using One-Stage Detector with a Coarse-to-Fine Attention.Diagnostics (Basel). 2022 Aug 7;12(8):1913. doi: 10.3390/diagnostics12081913. Diagnostics (Basel). 2022. PMID: 36010263 Free PMC article.
-
Determining Carina and Clavicular Distance-Dependent Positioning of Endotracheal Tube in Critically Ill Patients: An Artificial Intelligence-Based Approach.Biology (Basel). 2022 Mar 23;11(4):490. doi: 10.3390/biology11040490. Biology (Basel). 2022. PMID: 35453690 Free PMC article.
-
A novel training simulator for portable ultrasound identification of incorrect newborn endotracheal tube placement - observational diagnostic accuracy study protocol.BMC Pediatr. 2019 Nov 13;19(1):434. doi: 10.1186/s12887-019-1717-y. BMC Pediatr. 2019. PMID: 31722685 Free PMC article.
References
-
- Knapp S, Kofler J, Stoiser B, Thalhammer F, Burgmann H, Posch M, et al. The assessment of four different methods to verify tracheal tube placement in the critical care setting. Anesth Analg 1999;88:766-70. - PubMed
-
- Grmec S. Comparison of three different methods to confirm tracheal tube placement in emergency intubation. Intensive Care Med 2002;28:701-4. - PubMed
-
- Raphael DT, Benbassat M, Arnaudov D, Bohorquez A, Nasseri B. Validation study of two-microphone acoustic reflectometry for determination of breathing tube placement in 200 adult patients. Anesthesiology 2002;97:1371-7. - PubMed
-
- Owen RL, Cheney FW. Endobronchial intubation, a preventable complication. Anesthesiology 1987;67:255-7. - PubMed
-
- Morray J, Geiduschek J, Caplan R, Gild W, Cheney F. A comparison of pediatric and adult closed malpractice claims. Anesthesiology 1993;78:461-71. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical