

Phase III clinical trial development: a process of chutes and ladders
- PMID: 21062928
- PMCID: PMC3058405
- DOI: 10.1158/1078-0432.CCR-10-1273
Phase III clinical trial development: a process of chutes and ladders
Abstract
Purpose: The Institute of Medicine report on cooperative groups and the National Cancer Institute (NCI) report from the Operational Efficiency Working Group both recommend changes to the processes for opening a clinical trial. This article provides evidence for the need for such changes by completing the first comprehensive review of all the time and steps required to open a phase III oncology clinical trial and discusses the effect of time to protocol activation on subject accrual.
Methods: The Dilts and Sandler method was used at four cancer centers, two cooperative groups, and the NCI Cancer Therapy Evaluation Program. Accrual data were also collected.
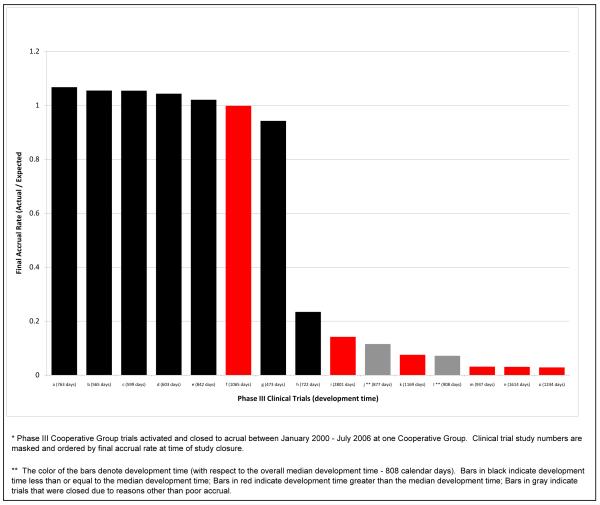
Results: Opening a phase III cooperative group therapeutic trial requires 769 steps, 36 approvals, and a median of approximately 2.5 years from formal concept review to study opening. Time to activation at one group ranged from 435 to 1,604 days, and time to open at one cancer center ranged from 21 to 836 days. At centers, group trials are significantly more likely to have zero accruals (38.8%) than nongroup trials (20.6%; P < 0.0001). Of the closed NCI Cancer Therapy Evaluation Program-approved phase III clinical trials from 2000 to 2007, 39.1% resulted in <21 accruals.
Conclusions: The length, variability, and low accrual results demonstrate the need for the NCI clinical trials system to be reengineered. Improvements will be of only limited effectiveness if done in isolation; there is a need to return to the collaborative spirit with all parties creating an efficient and effective system. Recommendations put forth by the Institute of Medicine and Operational Efficiency Working Group reports, if implemented, will aid this renewal.
©2010 AACR.
Figures

References
-
- IOM (Institute of Medicine), editor. A National Cancer Clinical Trials System for the 21st Century: Reinvigorating the NCI Cooperative Group Program. The National Academies Press; Washington, DC: 2010. - PubMed
-
- Gellhorn A. Invited remarks on the current state of research in clinical cancer. Cancer Chemotherapy Rep. 1959;5:1–12.
-
- Dilts DM, Sander AB. The “Invisible” Barriers to Clinical Trials: The impact of Structural, Infrastructural, and Procedural Barriers to Opening Oncology Clinical Trials. J Clin Oncol. 2006;24:454–52. - PubMed
-
- Dilts DM, Sander AB, Baker M, et al. Processes to Activate Phase III Clinical Trials in a Cooperative Oncology Group: The Case of the Cancer Leukemia Group B (CALGB) J Clin Oncol. 2006;24:4553–7. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
