

Synergistic enhancement of carboplatin efficacy with photodynamic therapy in a three-dimensional model for micrometastatic ovarian cancer
- PMID: 21062986
- PMCID: PMC3057933
- DOI: 10.1158/0008-5472.CAN-10-1783
Synergistic enhancement of carboplatin efficacy with photodynamic therapy in a three-dimensional model for micrometastatic ovarian cancer
Abstract
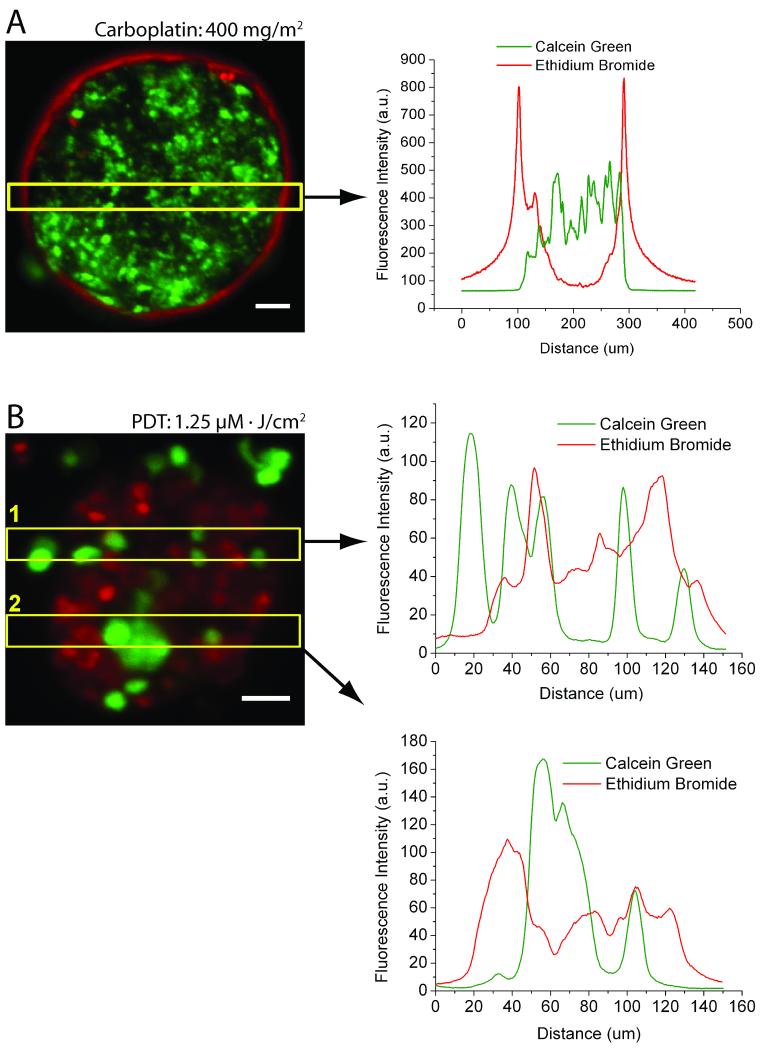
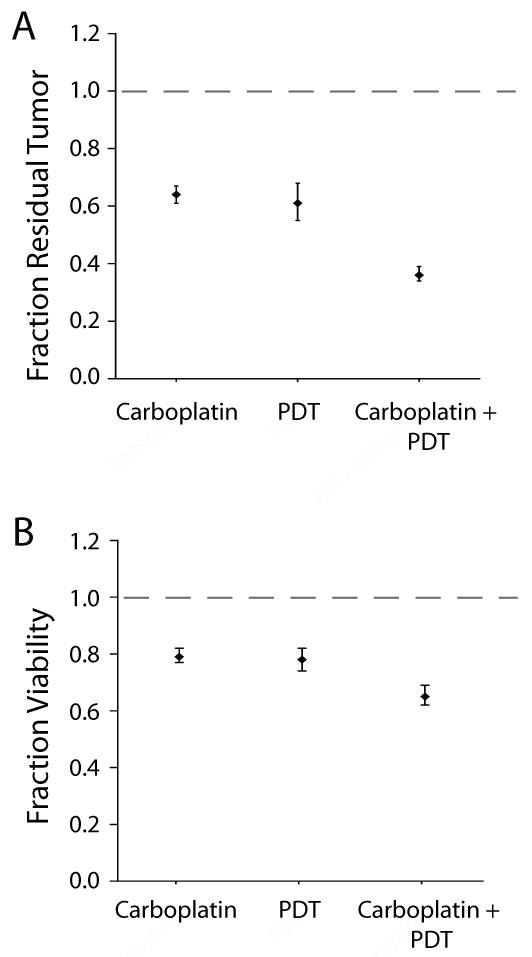
Metastatic ovarian cancer (OvCa) frequently recurs due to chemoresistance, highlighting the need for nonoverlapping combination therapies that mechanistically synergize to eradicate residual disease. Photodynamic therapy (PDT), a photochemistry-based cytotoxic modality, sensitizes ovarian tumors to platinum agents and biologics and has shown clinical promise against ovarian carcinomatosis. We introduce a three-dimensional (3D) model representing adherent ovarian micrometastases and high-throughput quantitative imaging methods to rapidly screen the order-dependent effects of combining benzoporphyrin-derivative (BPD) monoacid A-based PDT with low-dose carboplatin. 3D ovarian micronodules grown on Matrigel were subjected to BPD-PDT either before or after carboplatin treatment. We developed custom fluorescence image analysis routines to quantify residual tumor volume and viability. Carboplatin alone did not eradicate ovarian micrometastases at a dose of 400 mg/m2, leaving surviving cores that were nonsensitive or impermeable to chemotherapy. BPD-PDT (1.25 μmol/L·J/cm2) created punctate cytotoxic regions within tumors and disrupted micronodular structure. Treatment with BPD-PDT prior to low-dose carboplatin (40 mg/m2) produced a significant synergistic reduction [P<0.0001, analysis of covariance (ANCOVA)] in residual tumor volume [0.26; 95% confidence interval (95% CI), 0.19-0.36] compared with PDT alone (0.76; 95% CI, 0.63-0.92) or carboplatin alone (0.95; 95% CI, 0.83-1.09), relative to controls. This synergism was not observed with the reverse treatment order. Here, we demonstrate for the first time the use of a 3D model for micrometastatic OvCa as a rapid and quantitative reporter to optimize sequence and dosing regimens of clinically relevant combination strategies. This approach combining biological modeling with high-content imaging provides a platform to rapidly screen therapeutic strategies for a broad array of metastatic tumors.
Copyright © 2010 AACR.
Figures




References
-
- NAORA H, MONTELL DJ. OVARIAN CANCER METASTASIS: INTEGRATING INSIGHTS FROM DISPARATE MODEL ORGANISMS. NAT REV CANCER. 2005;5:355–66. - PubMed
-
- DEL CARMEN MG, RIZVI I, CHANG Y, et al. SYNERGISM OF EPIDERMAL GROWTH FACTOR RECEPTOR-TARGETED IMMUNOTHERAPY WITH PHOTODYNAMIC TREATMENT OF OVARIAN CANCER IN VIVO. JNCI. 2005;97:1516–24. - PubMed
-
- CHI DS, EISENHAUER EL, ZIVANOVIC O, et al. IMPROVED PROGRESSION-FREE AND OVERALL SURVIVAL IN ADVANCED OVARIAN CANCER AS A RESULT OF A CHANGE IN SURGICAL PARADIGM. GYNECOL ONCOL. 2009;114:26–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
