

Electrocardiologic and related methods of non-invasive detection and risk stratification in myocardial ischemia: state of the art and perspectives
- PMID: 21063467
- PMCID: PMC2975259
- DOI: 10.3205/000116
Electrocardiologic and related methods of non-invasive detection and risk stratification in myocardial ischemia: state of the art and perspectives
Abstract
Background: Electrocardiographic methods still provide the bulk of cardiovascular diagnostics. Cardiac ischemia is associated with typical alterations in cardiac biosignals that have to be measured, analyzed by mathematical algorithms and allegorized for further clinical diagnostics. The fast growing fields of biomedical engineering and applied sciences are intensely focused on generating new approaches to cardiac biosignal analysis for diagnosis and risk stratification in myocardial ischemia.
Objectives: To present and review the state of the art in and new approaches to electrocardiologic methods for non-invasive detection and risk stratification in coronary artery disease (CAD) and myocardial ischemia; secondarily, to explore the future perspectives of these methods.
Methods: In follow-up to the Expert Discussion at the 2008 Workshop on "Biosignal Analysis" of the German Society of Biomedical Engineering in Potsdam, Germany, we comprehensively searched the pertinent literature and databases and compiled the results into this review. Then, we categorized the state-of-the-art methods and selected new approaches based on their applications in detection and risk stratification of myocardial ischemia. Finally, we compared the pros and cons of the methods and explored their future potentials for cardiology.
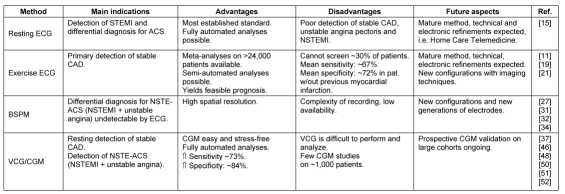
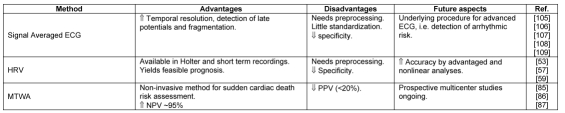
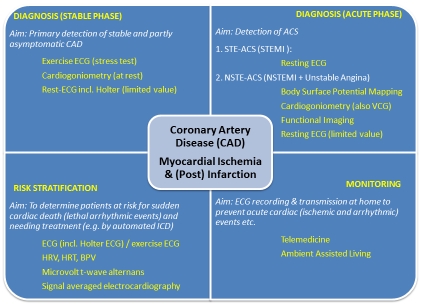
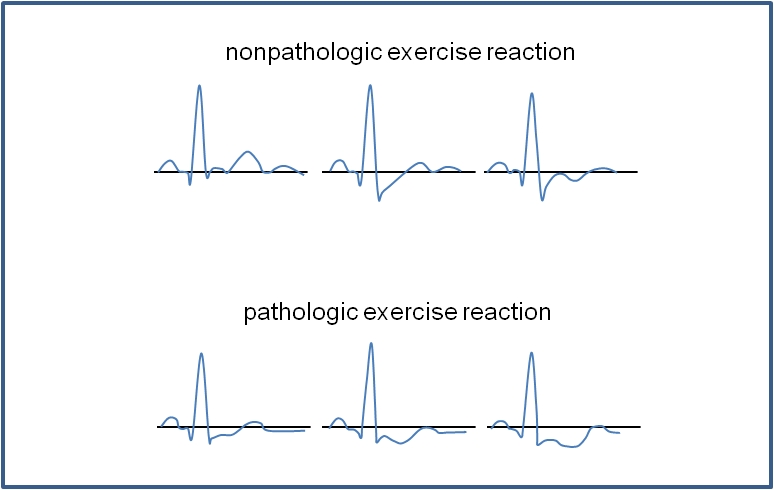
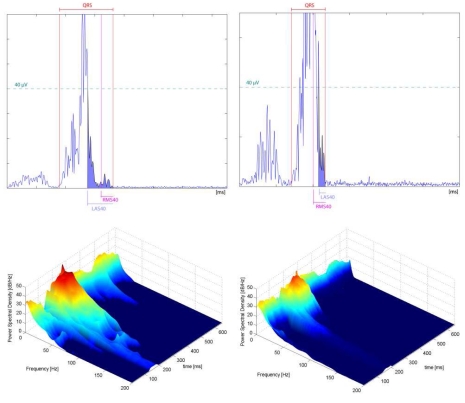
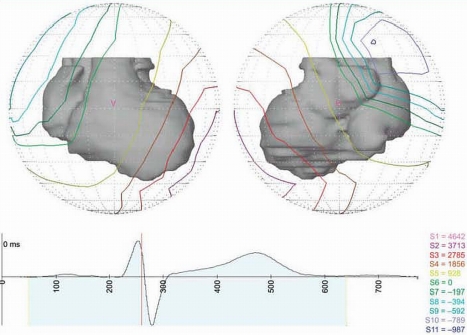
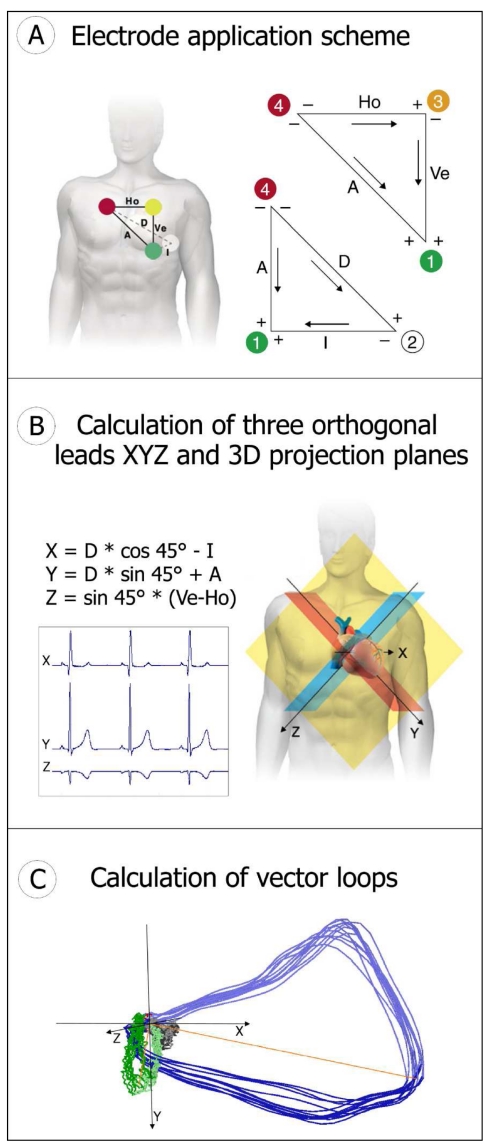
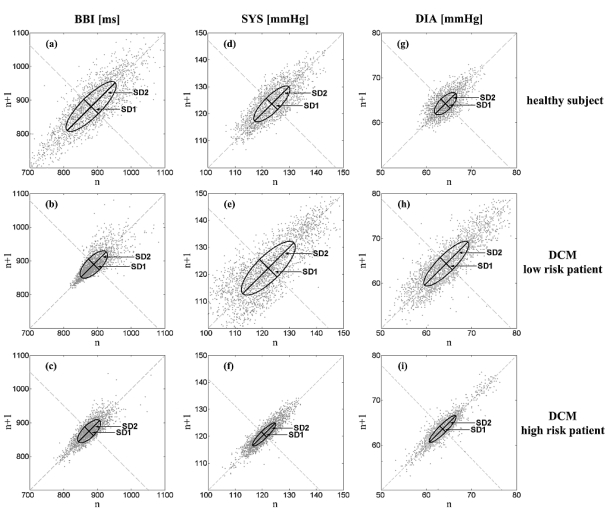
Results: Resting ECG, particularly suited for detecting ST-elevation myocardial infarctions, and exercise ECG, for the diagnosis of stable CAD, are state-of-the-art methods. New exercise-free methods for detecting stable CAD include cardiogoniometry (CGM); methods for detecting acute coronary syndrome without ST elevation are Body Surface Potential Mapping, functional imaging and CGM. Heart rate variability and blood pressure variability analyses, microvolt T-wave alternans and signal-averaged ECG mainly serve in detecting and stratifying the risk for lethal arrythmias in patients with myocardial ischemia or previous myocardial infarctions. Telemedicine and ambient-assisted living support the electrocardiological monitoring of at-risk patients.
Conclusions: There are many promising methods for the exercise-free, non-invasive detection of CAD and myocardial ischemia in the stable and acute phases. In the coming years, these new methods will help enhance state-of-the-art procedures in routine diagnostics. The future can expect that equally novel methods for risk stratification and telemedicine will transition into clinical routine.
Hintergrund: Elektrokardiografische Verfahren stellen nach wie vor die primär wichtigsten Methoden zur kardiologischen Diagnostik dar. Eine Herzischämie geht mit typischen Veränderungen kardialer Biosignale einher, die anhand mathematischer Algorithmen analysiert und für den weiteren klinischen Pfad aufbereitet werden müssen. Die rasant wachsende Biomedizintechnik sowie angewandte Wissenschaften beschäftigen sich intensiv mit neuen Ansätzen zur Auswertung kardialer Biosignale zur Ischämiediagnostik und Risikostratifizierung.
Ziele: Hauptziel dieser Übersichtsarbeit ist es, den gegenwärtigen Stand der Technik sowie neue Ansätze im Bereich elektrokardiologischer Verfahren zur nicht-invasiven Erkennung und Risikostratifizierung von koronarer Herzkrankheit (KHK) und Myokardischämie vorzustellen und zu bewerten. Als Sekundärziel werden die Zukunftsperspektiven dieser Verfahren aufgezeigt.
Methoden: Beginnend mit Expertendiskussionen während des Workshops „Biosignalverarbeitung“ der Deutschen Gesellschaft für Biomedizinische Technik (2008 in Potsdam) sowie anschließenden intensiven Recherchen der Literatur und Datenbanken wurde dieser Review erstellt. Es erfolgte eine Kategorisierung von Verfahren des Standes der Technik sowie ausgewählter neuer Ansätze entsprechend ihrer Einsatzgebiete zur Ischämiediagnostik und Risikostratifizierung. Die Vor- und Nachteile wurden aufgezeigt und die künftigen Möglichkeiten dieser Verfahren in der Kardiologie untersucht.
Ergebnisse: Als Stand der Technik anzusehen ist das Ruhe-EKG (insbesondere geeignet für Erkennung von ST-Hebungsinfarkten) und das Belastungs-EKG (Diagnostik von stabiler KHK). Neue belastungsfreie Verfahren zur Erkennung von stabiler KHK sind die Kardiogoniometrie (KGM) sowie zur Erkennung des Akuten Koronarsyndroms ohne ST-Hebung das Body Surface Potential Mapping, Funktionelle Bildgebung sowie die KGM. Analyse von Herzfrequenz- und Blutdruckvariabilität, T-Wellen-Alternans und Spätpotentialen dienen vorrangig der Erkennung und Stratifizierung des Risikos für letale Arrythmien bei Patienten mit Myokardischämie oder nach durchlebtem Myokardinfarkt. Telemedizin und technologieunterstütztes Wohnen (Ambient Assisted Living) unterstützen das elektrokardiologische Monitoring von Risikopatienten.
Schlussfolgerungen: Es gibt vielversprechende Ansätzen insbesondere zur belastungsfreien nichtinvasiven Erkennung von KHK und Myokardischämie in stabiler Phase und Akutsituation, welche in den nächsten Jahren die Standardverfahren in der Routinediagnostik ergänzen werden. Ebenso neue Verfahren der Risikostratifizierung sowie telemedizinische Techniken werden den Übergang in die Routineanwendung finden.
Keywords: body surface potential mapping; cardiogoniometry; exercise electrocardiography; functional imaging; heart rate variability; resting electrocardiography.
Figures
Similar articles
-
API expert consensus document on management of ischemic heart disease.J Assoc Physicians India. 2006 Jun;54:469-80. J Assoc Physicians India. 2006. PMID: 16909697 Review.
-
High-frequency QRS analysis improves the specificity of exercise ECG testing in women referred for angiography.J Electrocardiol. 2013 Jan-Feb;46(1):19-26. doi: 10.1016/j.jelectrocard.2012.08.007. J Electrocardiol. 2013. PMID: 23312358
-
Olson method for locating and calculating the extent of transmural ischemic areas at risk of infarction.J Electrocardiol. 2014 Jul-Aug;47(4):430-7. doi: 10.1016/j.jelectrocard.2014.04.005. Epub 2014 Apr 26. J Electrocardiol. 2014. PMID: 24850318
-
Electrocardiographic ST-segment changes during acute myocardial ischemia.Card Electrophysiol Rev. 2002 Sep;6(3):196-203. doi: 10.1023/a:1016352205286. Card Electrophysiol Rev. 2002. PMID: 12114838 Review.
-
Electrocardiographic body surface mapping: potential tool for the detection of transient myocardial ischemia in the 21st century?Ann Noninvasive Electrocardiol. 2009 Apr;14(2):201-10. doi: 10.1111/j.1542-474X.2009.00284.x. Ann Noninvasive Electrocardiol. 2009. PMID: 19419406 Free PMC article. Review.
Cited by
-
Detection of Acute Myocardial Infarction in a Pig Model Using the SAN-Atrial-AVN-His (SAAH) Electrocardiogram (ECG), Model PHS-A10, an Automated and Integrated Signals Recognition System.Med Sci Monit. 2018 Mar 4;24:1303-1309. doi: 10.12659/msm.905961. Med Sci Monit. 2018. PMID: 29502127 Free PMC article.
-
Role of exercise cardiogoniometry in coronary artery disease diagnostics.Clin Res Cardiol. 2017 Aug;106(8):573-581. doi: 10.1007/s00392-017-1087-0. Epub 2017 Mar 13. Clin Res Cardiol. 2017. PMID: 28289841
-
Sensitivity of epicardial electrical markers to acute ischemia detection.J Electrocardiol. 2014 Nov-Dec;47(6):836-41. doi: 10.1016/j.jelectrocard.2014.08.014. Epub 2014 Aug 17. J Electrocardiol. 2014. PMID: 25242529 Free PMC article.
-
Cardiogoniometry as a diagnostic tool in patients with acute coronary syndromes: results of the CGM@ACS trial.Clin Res Cardiol. 2012 Sep;101(9):727-36. doi: 10.1007/s00392-012-0452-2. Epub 2012 Apr 7. Clin Res Cardiol. 2012. PMID: 22485015 Free PMC article.
-
The predictive value of Cardiodynamicsgram in myocardial perfusion abnormalities.PLoS One. 2018 Dec 17;13(12):e0208859. doi: 10.1371/journal.pone.0208859. eCollection 2018. PLoS One. 2018. PMID: 30557346 Free PMC article.
References
-
- Einthoven W. Herinneringsbundel Professor S.S. Rosenstein. Leiden: Eduard Ijdo; 1902. Galvanometrische registratie van het menschilijk electrocardiogram; pp. 101–107.
-
- Cooper JK. Electrocardiography 100 years ago. Origins, pioneers and contributors. N Engl J Med. 1986;315:461–464. doi: 10.1056/NEJM198608143150722. Available from: http://dx.doi.org/10.1056/NEJM198608143150722. - DOI - DOI - PubMed
-
- Priori SG, Aliot E, Blomstrom-Lundqvist C, Bossaert L, Breithardt G, Brugada P, Camm AJ, Cappato R, Cobbe SM, Di Mario C, Maron BJ, McKenna WJ, Pedersen AK, Ravens U, Schwartz PJ, Trusz-Gluza M, Vardas P, Wellens HJ, Zipes DP. Task Force on Sudden Cardiac Death of the European Society of Cardiology. Eur Heart J. 2001;22(16):1374–1450. doi: 10.1053/euhj.2001.2824. Available from: http://dx.doi.org/10.1053/euhj.2001.2824. - DOI - DOI - PubMed
-
- De Vreede-Swagemakers JJ, Gorgels AP, Dubois-Arbouw WI, van Ree JW, Daemen MJAP, Houben LGE, Wellens HJJ. Out-of-hospital cardiac arrest in the 1990's: a population-based study in the Maastricht area on incidence, characteristics and survival. J Am Coll Cardiol. 1997;30(6):1500–1505. doi: 10.1016/S0735-1097(97)00355-0. Available from: http://dx.doi.org/10.1016/S0735-1097(97)00355-0. - DOI - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
