

Seronegative necrolytic acral erythema: a distinct clinical subset?
- PMID: 21063519
- PMCID: PMC2965913
- DOI: 10.4103/0019-5154.70676
Seronegative necrolytic acral erythema: a distinct clinical subset?
Abstract
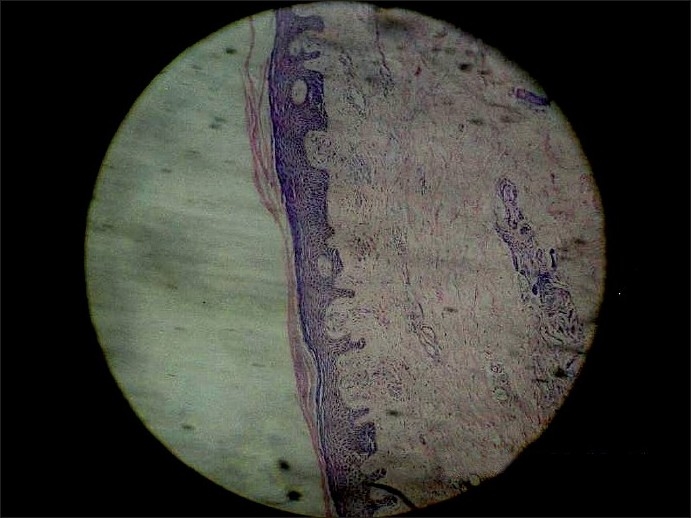
A patient was referred to us with asymptomatic, erythematous, nonitchy, scaly lesions present bilaterally on the dorsa of his feet and toes since the last 2 months. Both the legs had pitting edema as well. There were hyperkeratosis, focal parakeratosis, acanthosis and scattered spongiosis in the epidermis, and proliferation of capillaries with perivascular infiltration of lymphomononuclear cells in the dermis. There was no serological evidence of hepatitis C virus. Laboratory investigations revealed hypoalbuminemia and low-normal serum zinc. On clinicopathological correlation, we made a diagnosis of necrolytic acral erythema (NAE). The lesions responded dramatically to oral zinc sulfate and topical clobetasol propionate within 3 weeks with disappearance of edema and scaling and only a minimal residual erythema. This is the first reported case of NAE from Eastern India. NAE with negative serology for hepatitis C may be viewed as a distinct subset of the condition that had been originally described.
Keywords: Acral erythema; hepatitis C; necrolytic erythema; oral zinc.
Conflict of interest statement
Figures


References
-
- el Darouti M, Abu el Ela M. Neorolytic acral erythema: A cutaneous marker of viral hepatitis C. Int J Dermatol. 1996;35:252–6. - PubMed
-
- Frank C, Mohamed MK, Strickland GT, Lavanchy D, Arthur RR, Magder LS, et al. The role of parenteral antischistosomal therapy in the spread of hepatitis C virus in Egypt. Lancet. 2000;355:887–91. - PubMed
-
- Geria AN, Holcomb KZ, Scheinfeld NS. Necrolytic acral erythema: A review of the literature. Cutis. 2009;83:309–14. - PubMed
-
- Liu A, Erickson CP, Cockerell CJ, Hsu S. Necrolytic acral erythema: A case not associated with hepatitis C infection. Dermatol Online J. 2008;14:10. - PubMed
-
- Wu YH, Tu ME, Lee CS, Lin YC. Necrolytic acral erythema without hepatitis C infection. J Cutan Pathol. 2009;36:355–8. - PubMed
LinkOut - more resources
Full Text Sources