Acute gastric dilatation in a patient with anorexia nervosa binge/purge subtype
- PMID: 21063567
- PMCID: PMC2966577
- DOI: 10.4103/0974-2700.70774
Acute gastric dilatation in a patient with anorexia nervosa binge/purge subtype
Abstract
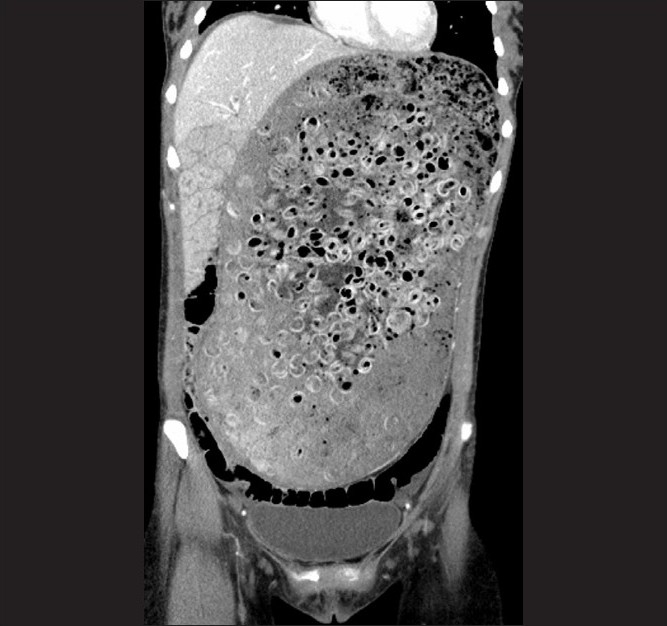
Acute gastric dilatation is a rare complication of anorexia nervosa binge/purge subtype that results from gastrointestinal abnormalities, including decreased gastric motility and delayed gastric emptying. Early diagnosis and intervention is critical since delay may result in gastric necrosis, perforation, shock, and death. We report a 26-year-old female with anorexia nervosa binge/purge subtype, who presented with abdominal pain and nausea after a binge episode. Abdominal radiography and computed tomography showed a grossly dilated stomach measuring 32 cm × 17.9 cm consistent with acute gastric dilatation. She underwent exploratory laparotomy with gastrotomy and gastric decompression, and recovered uneventfully. Initially, the patient denied the binge episode, as many patients with eating disorders do, but later revealed an extensive history of anorexia nervosa binge/purge subtype. This case stresses the importance of obtaining a thorough history of eating disorders and maintaining a high index of suspicion for acute gastric dilatation in young women who present with abdominal pain and distention.
Keywords: Acute gastric dilatation; anorexia; binge/purge; denial; eating disorder; gastric dysmotility.
Conflict of interest statement
Figures

References
-
- Hadley SJ, Walsh BT. Gastrointestinal disturbances in anorexia nervosa and bulimia nervosa. Curr Drug Targets CNS Neurol Disord. 2003;2:1–9. - PubMed
-
- Turan M, Sen M, Canbay E, Karadayi K, Yildiz E. Gastric necrosis and perforation caused by acute gastric dilatation: report of a case. Surg Today. 2003;33:302–4. - PubMed
-
- Nakao A, Isozaki H, Iwagaki H, Kanagawa T, Takakura N, Tanaka N. Gastric perforation caused by a bulimic attack in an anorexia nervosa patient: report of a case. Surg Today. 2000;30:435–7. - PubMed
-
- Watanabe S, Terazawa K, Asari M, Matsubara K, Shiono H, Shimizu K. An autopsy case of sudden death due to acute gastric dilatation without rupture. Forensic Sci Int. 2008;180:6–10. - PubMed