

A balanced view of balanced solutions
- PMID: 21067552
- PMCID: PMC3219243
- DOI: 10.1186/cc9230
A balanced view of balanced solutions
Abstract
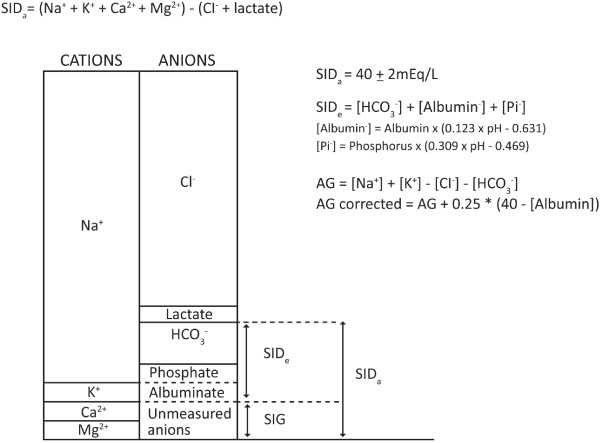
The present review of fluid therapy studies using balanced solutions versus isotonic saline fluids (both crystalloids and colloids) aims to address recent controversy in this topic. The change to the acid-base equilibrium based on fluid selection is described. Key terms such as dilutional-hyperchloraemic acidosis (correctly used instead of dilutional acidosis or hyperchloraemic metabolic acidosis to account for both the Henderson-Hasselbalch and Stewart equations), isotonic saline and balanced solutions are defined. The review concludes that dilutional-hyperchloraemic acidosis is a side effect, mainly observed after the administration of large volumes of isotonic saline as a crystalloid. Its effect is moderate and relatively transient, and is minimised by limiting crystalloid administration through the use of colloids (in any carrier). Convincing evidence for clinically relevant adverse effects of dilutional-hyperchloraemic acidosis on renal function, coagulation, blood loss, the need for transfusion, gastrointestinal function or mortality cannot be found. In view of the long-term use of isotonic saline either as a crystalloid or as a colloid carrier, the paucity of data documenting detrimental effects of dilutional-hyperchloraemic acidosis and the limited published information on the effects of balanced solutions on outcome, we cannot currently recommend changing fluid therapy to the use of a balanced colloid preparation.
Figures
Comment in
-
Isotonic saline--the only solution to recommend?Crit Care. 2011 Feb 14;15(1):404; author reply 404. doi: 10.1186/cc10008. Crit Care. 2011. PMID: 21371357 Free PMC article. No abstract available.
References
-
- Powell-Tuck J, Gosling P, Lobo DN, Allison SP, Carlson GL, Gore M, Lewington AJ, Pearse RM, Mythen MG. British Consensus Guidelines on Intravenous Fluid Therapy for Adult Surgical Patients (GIFTASUP) London: NHS National Library of Health; 2009.
-
- Hasselbalch KA. Die berechnung der wasserstoffzahl des blutes auf der freien und gebundenen kohlensaure desselben, und die sauerstoff bindung des blutes als funktion der wasserstoffzahl. Biochem Z. 1916;78:112–144.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
