

The cross-sectional GRAS sample: a comprehensive phenotypical data collection of schizophrenic patients
- PMID: 21067598
- PMCID: PMC3002316
- DOI: 10.1186/1471-244X-10-91
The cross-sectional GRAS sample: a comprehensive phenotypical data collection of schizophrenic patients
Abstract
Background: Schizophrenia is the collective term for an exclusively clinically diagnosed, heterogeneous group of mental disorders with still obscure biological roots. Based on the assumption that valuable information about relevant genetic and environmental disease mechanisms can be obtained by association studies on patient cohorts of ≥ 1000 patients, if performed on detailed clinical datasets and quantifiable biological readouts, we generated a new schizophrenia data base, the GRAS (Göttingen Research Association for Schizophrenia) data collection. GRAS is the necessary ground to study genetic causes of the schizophrenic phenotype in a 'phenotype-based genetic association study' (PGAS). This approach is different from and complementary to the genome-wide association studies (GWAS) on schizophrenia.
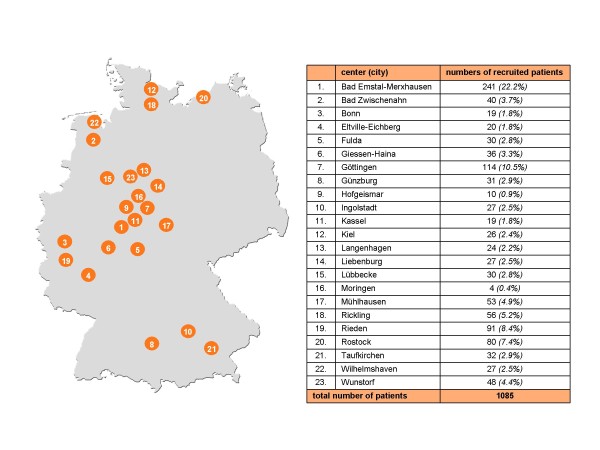
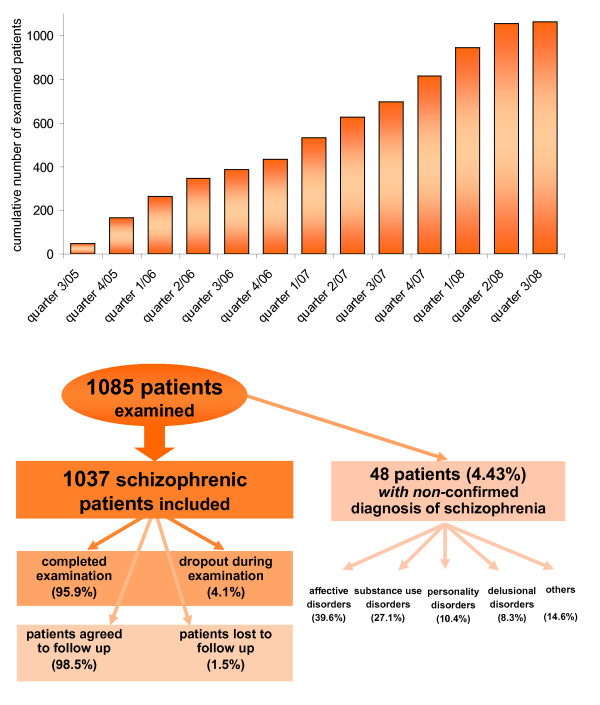
Methods: For this purpose, 1085 patients were recruited between 2005 and 2010 by an invariable team of traveling investigators in a cross-sectional field study that comprised 23 German psychiatric hospitals. Additionally, chart records and discharge letters of all patients were collected.
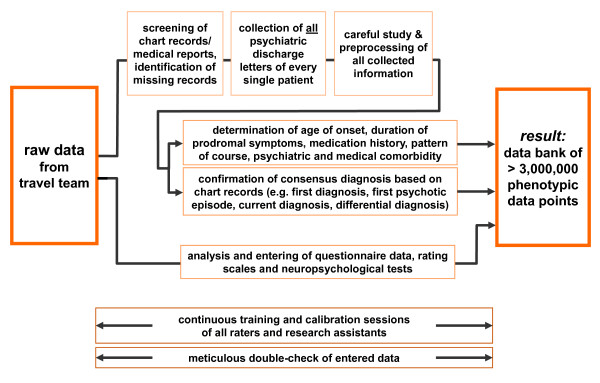
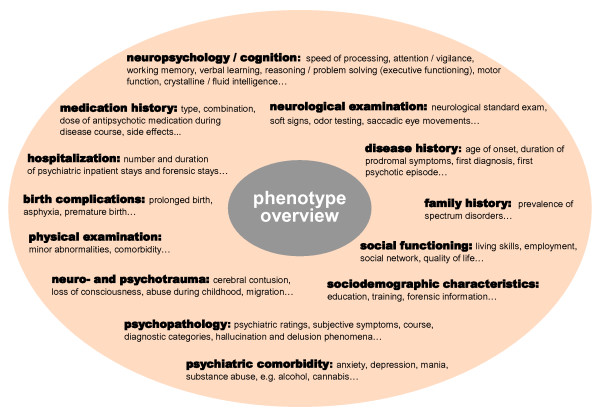
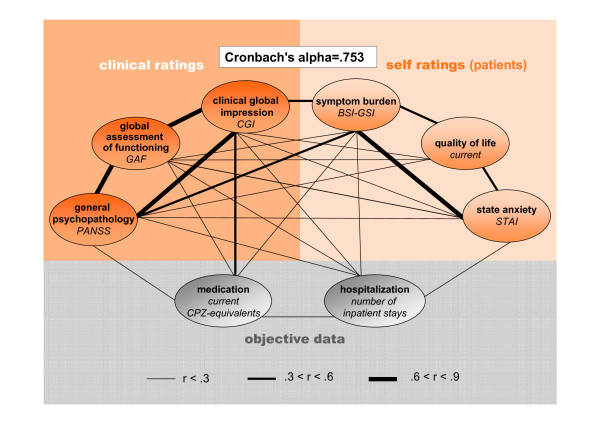
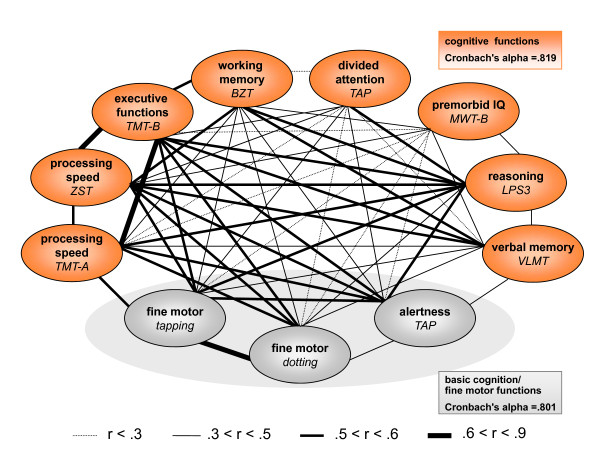
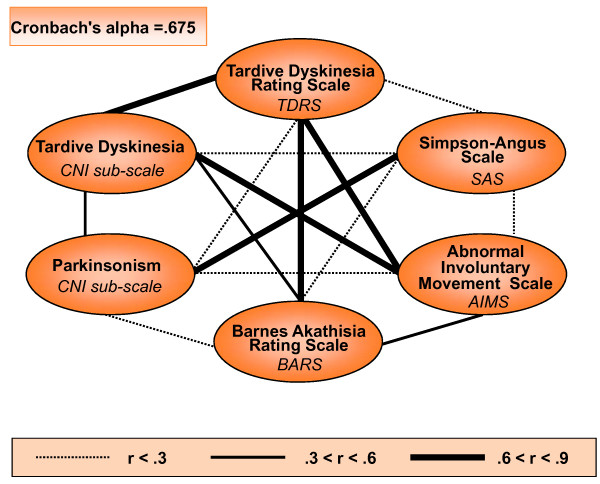
Results: The corresponding dataset extracted and presented in form of an overview here, comprises biographic information, disease history, medication including side effects, and results of comprehensive cross-sectional psychopathological, neuropsychological, and neurological examinations. With >3000 data points per schizophrenic subject, this data base of living patients, who are also accessible for follow-up studies, provides a wide-ranging and standardized phenotype characterization of as yet unprecedented detail.
Conclusions: The GRAS data base will serve as prerequisite for PGAS, a novel approach to better understanding 'the schizophrenias' through exploring the contribution of genetic variation to the schizophrenic phenotypes.
Figures

Similar articles
-
Modification of cognitive performance in schizophrenia by complexin 2 gene polymorphisms.Arch Gen Psychiatry. 2010 Sep;67(9):879-88. doi: 10.1001/archgenpsychiatry.2010.107. Arch Gen Psychiatry. 2010. PMID: 20819981
-
[Phenotype-based genetic association studies (PGAS): a new approach to understanding the genotype contribution to schizophrenic phenotypes].Fortschr Neurol Psychiatr. 2013 May;81(5):240-2. doi: 10.1055/s-0033-1335157. Epub 2013 May 21. Fortschr Neurol Psychiatr. 2013. PMID: 23695788 German.
-
Phenotype-Based Genetic Association Studies (PGAS)-Towards Understanding the Contribution of Common Genetic Variants to Schizophrenia Subphenotypes.Genes (Basel). 2014 Feb 27;5(1):97-105. doi: 10.3390/genes5010097. Genes (Basel). 2014. PMID: 24705289 Free PMC article.
-
Cognitive impairment as a target for pharmacological treatment in schizophrenia.Schizophr Res. 1995 Sep;17(1):123-9. doi: 10.1016/0920-9964(95)00037-m. Schizophr Res. 1995. PMID: 8541245 Review. No abstract available.
-
Will the novel antipsychotics significantly ameliorate neuropsychological deficits and improve adaptive functioning in schizophrenia?Psychol Med. 1999 Jan;29(1):1-8. doi: 10.1017/s0033291798006990. Psychol Med. 1999. PMID: 10077288 Review. No abstract available.
Cited by
-
Study protocol of the Berlin Research Initiative for Diagnostics, Genetics and Environmental Factors in Schizophrenia (BRIDGE-S).BMC Psychiatry. 2023 Jan 12;23(1):31. doi: 10.1186/s12888-022-04447-4. BMC Psychiatry. 2023. PMID: 36635663 Free PMC article.
-
A CAG repeat polymorphism of KCNN3 predicts SK3 channel function and cognitive performance in schizophrenia.EMBO Mol Med. 2011 Jun;3(6):309-19. doi: 10.1002/emmm.201100135. Epub 2011 Mar 24. EMBO Mol Med. 2011. PMID: 21433290 Free PMC article.
-
A normal genetic variation modulates synaptic MMP-9 protein levels and the severity of schizophrenia symptoms.EMBO Mol Med. 2017 Aug;9(8):1100-1116. doi: 10.15252/emmm.201707723. EMBO Mol Med. 2017. PMID: 28623238 Free PMC article.
-
Common variants of the genes encoding erythropoietin and its receptor modulate cognitive performance in schizophrenia.Mol Med. 2012 Sep 7;18(1):1029-40. doi: 10.2119/molmed.2012.00190. Mol Med. 2012. PMID: 22669473 Free PMC article.
-
Genome-wide association study results for educational attainment aid in identifying genetic heterogeneity of schizophrenia.Nat Commun. 2018 Aug 6;9(1):3078. doi: 10.1038/s41467-018-05510-z. Nat Commun. 2018. PMID: 30082721 Free PMC article.
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders, (DSM-IV) 4. Washington, DC: American Psychiatric Press; 1994.
-
- World Health Organization. The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and diagnostic guidelines. Geneva: WHO; 1992.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
