

Current practices in treatment of female genital fistula: a cross sectional study
- PMID: 21067606
- PMCID: PMC2995487
- DOI: 10.1186/1471-2393-10-73
Current practices in treatment of female genital fistula: a cross sectional study
Abstract
Background: Maternal outcomes in most countries of the developed world are good. However, in many developing/resource-poor countries, maternal outcomes are bleaker: Every year, more than 500,000 women die in childbirth, mostly in resource-poor countries. Those who survive often suffer from severe and long-term morbidities. One of the most devastating injuries is obstetric fistula, occurring most often in south Asia and sub-Saharan Africa. Fistula treatment and care are available in many countries across Africa and Asia, but there is a lack of reliable data around clinical factors associated with the success of fistula repair surgery. Most published research has been retrospective. While these studies have provided useful information about the care and treatment of fistula, they are limited by the design. This study was designed to identify practices in care that could lead to the design of prospective and randomized controlled trials.
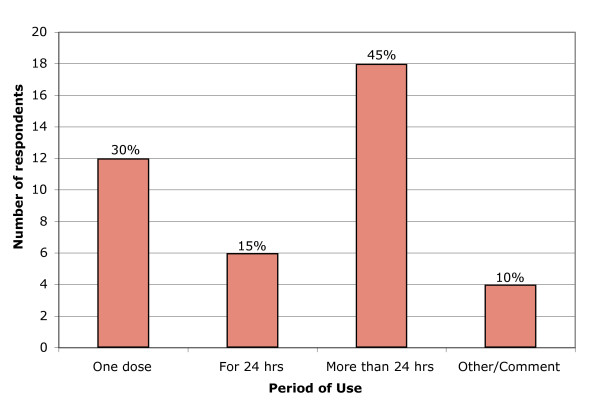
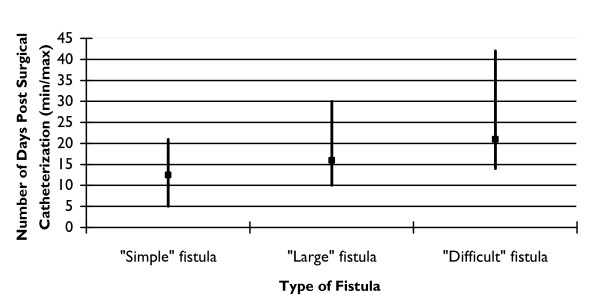
Methods: Self-administered questionnaires were completed by 40 surgeons known to provide fistula treatment services in Africa and Asia at private and government hospitals. The questionnaire was divided into three parts to address the following issues: prophylactic use of antibiotics before, during, and after fistula surgery; urethral catheter management; and management practices for patients with urinary incontinence following fistula repair.
Results: The results provide a glimpse into current practices in fistula treatment and care across a wide swath of geographic, economic, and organizational considerations. There is consensus in treatment in some areas (routine use of prophylactic antibiotics, limited bed rest until the catheter is removed, nonsurgical treatment for postsurgical incontinence), while there are wide variations in practice in other areas (duration of catheter use, surgical treatments for postsurgical incontinence). These findings are based on a small sample and do not allow for recommending changes in clinical care, but they point to issues for possible clinical trial research that would contribute to more efficient and effective fistula care.
Conclusions: The findings from the survey allowed us to consider clinical practices most influential in the cost, efficacy, and safety of fistula treatment. These considerations led us to formulate recommendations for eight randomized controlled trials on the following subjects: 1) Efficacy/safety of short-term catheterization; 2) efficacy of surgical and nonsurgical therapies for urinary incontinence; 3) technical measures during fistula repair to reduce the incidence of post-surgery incontinence; 4) identification of predictive factors for "incurable fistula"; 5) usefulness of urodynamic studies in the management of urinary incontinence; 6) incidence and significance of multi-drug resistant bacteria in the fistula population; 7) primary management of small, new fistulas by catheter drainage; and 8) antibiotic prophylaxis in fistula repair.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
