

Intensive lowering of LDL cholesterol with 80 mg versus 20 mg simvastatin daily in 12,064 survivors of myocardial infarction: a double-blind randomised trial
- PMID: 21067805
- PMCID: PMC2988223
- DOI: 10.1016/S0140-6736(10)60310-8
Intensive lowering of LDL cholesterol with 80 mg versus 20 mg simvastatin daily in 12,064 survivors of myocardial infarction: a double-blind randomised trial
Erratum in
- Lancet. 2011 Jan 8;377(9760):126
Abstract
Background: Lowering of LDL cholesterol reduces major vascular events, but whether more intensive therapy safely produces extra benefits is uncertain. We aimed to establish efficacy and safety of more intensive statin treatment in patients at high cardiovascular risk.
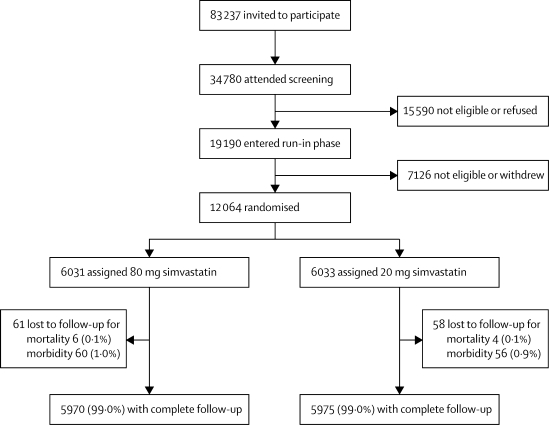
Methods: We undertook a double-blind randomised trial in 12,064 men and women aged 18-80 years with a history of myocardial infarction. Participants were either currently on or had clear indication for statin therapy, and had a total cholesterol concentration of at least 3·5 mmol/L if already on a statin or 4·5 mmol/L if not. Randomisation to either 80 mg or 20 mg simvastatin daily was done centrally using a minimisation algorithm. Participants were assessed at 2, 4, 8, and 12 months after randomisation and then every 6 months until final follow-up. The primary endpoint was major vascular events, defined as coronary death, myocardial infarction, stroke, or arterial revascularisation. Analysis was by intention to treat. This study is registered, number ISRCTN74348595.
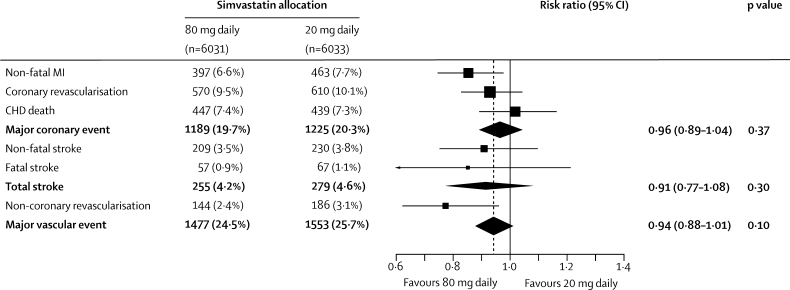
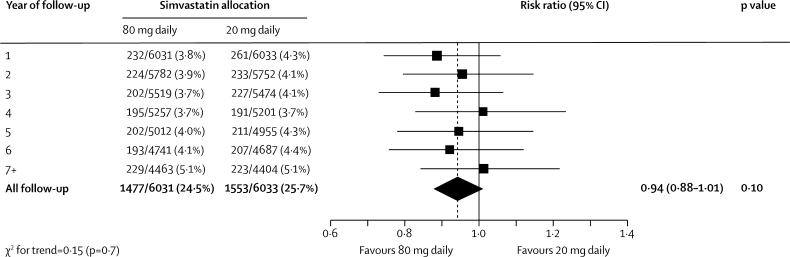
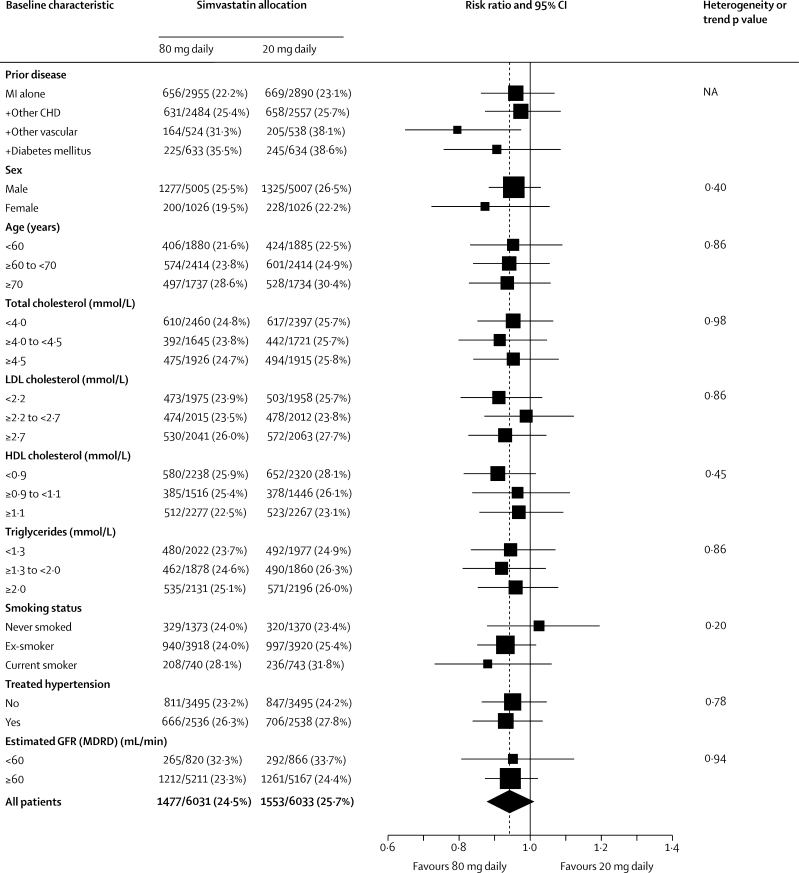
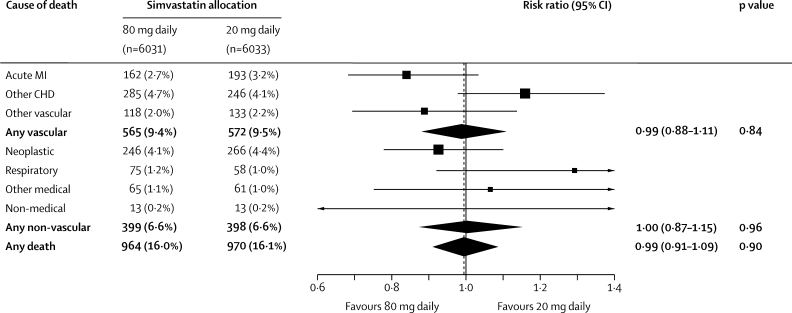
Findings: 6031 participants were allocated 80 mg simvastatin daily, and 6033 allocated 20 mg simvastatin daily. During a mean follow-up of 6·7 (SD 1·5) years, allocation to 80 mg simvastatin produced an average 0·35 (SE 0·01) mmol/L greater reduction in LDL cholesterol compared with allocation to 20 mg. Major vascular events occurred in 1477 (24·5%) participants allocated 80 mg simvastatin versus 1553 (25·7%) of those allocated 20 mg, corresponding to a 6% proportional reduction (risk ratio 0·94, 95% CI 0·88-1·01; p=0·10). There were no apparent differences in numbers of haemorrhagic strokes (24 [0·4%] vs 25 [0·4%]) or deaths attributed to vascular (565 [9·4%] vs 572 [9·5%]) or non-vascular (399 [6·6%] vs 398 [6·6%]) causes. Compared with two (0·03%) cases of myopathy in patients taking 20 mg simvastatin daily, there were 53 (0·9%) cases in the 80 mg group.
Interpretation: The 6% (SE 3·5%) reduction in major vascular events with a further 0·35 mmol/L reduction in LDL cholesterol in our trial is consistent with previous trials. Myopathy was increased with 80 mg simvastatin daily, but intensive lowering of LDL cholesterol can be achieved safely with other regimens.
Funding: Merck; The Clinical Trial Service Unit also receives funding from the UK Medical Research Council and the British Heart Foundation.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Is intensive LDL-cholesterol lowering beneficial and safe?Lancet. 2010 Nov 13;376(9753):1622-4. doi: 10.1016/S0140-6736(10)61545-0. Epub 2010 Nov 8. Lancet. 2010. PMID: 21067806 No abstract available.
References
-
- Stamler J, Vaccaro O, Neaton JD, Wentworth D. Diabetes, other risk factors, and 12-yr cardiovascular mortality for men screened in the Multiple Risk Factor Intervention Trial. Diabetes Care. 1993;16:434–444. - PubMed
-
- Cholesterol Treatment Trialists' Collaboration Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90 056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. - PubMed
-
- Heart Protection Study Collaborative Group MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20 536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360:7–22.
-
- Cannon CP, Braunwald E, McCabe CH. Intensive versus moderate lipid lowering with statins after acute coronary syndromes. N Engl J Med. 2004;350:1495–1504. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
