

Mechanisms of reflex bladder activation by pudendal afferents
- PMID: 21068196
- PMCID: PMC3043805
- DOI: 10.1152/ajpregu.00154.2010
Mechanisms of reflex bladder activation by pudendal afferents
Abstract
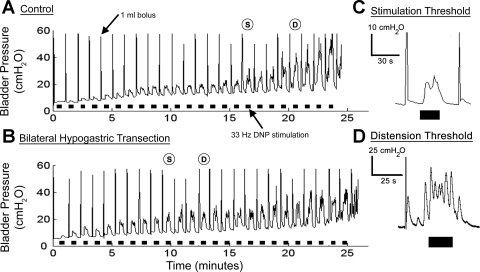
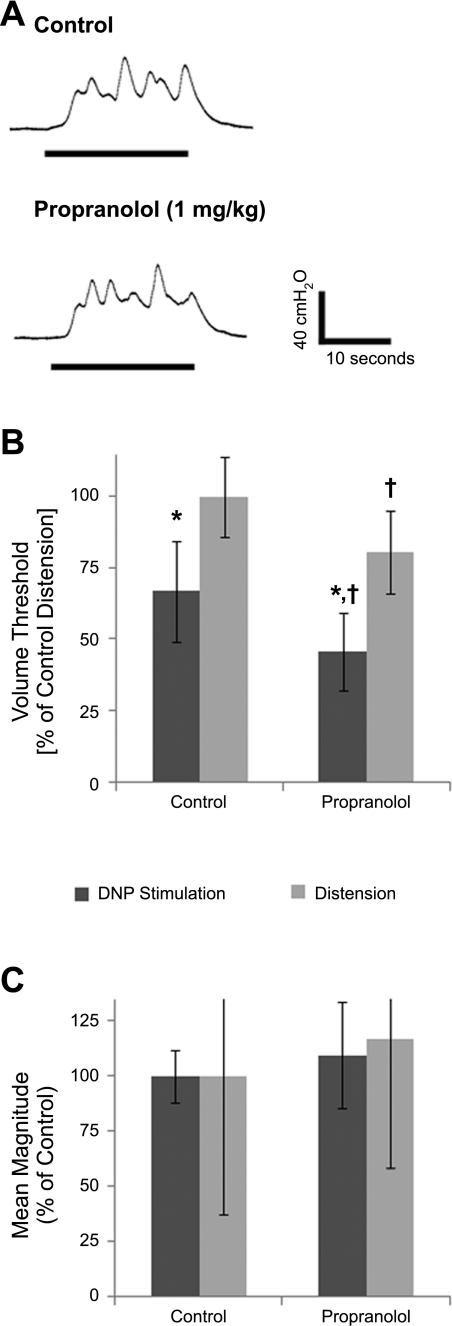
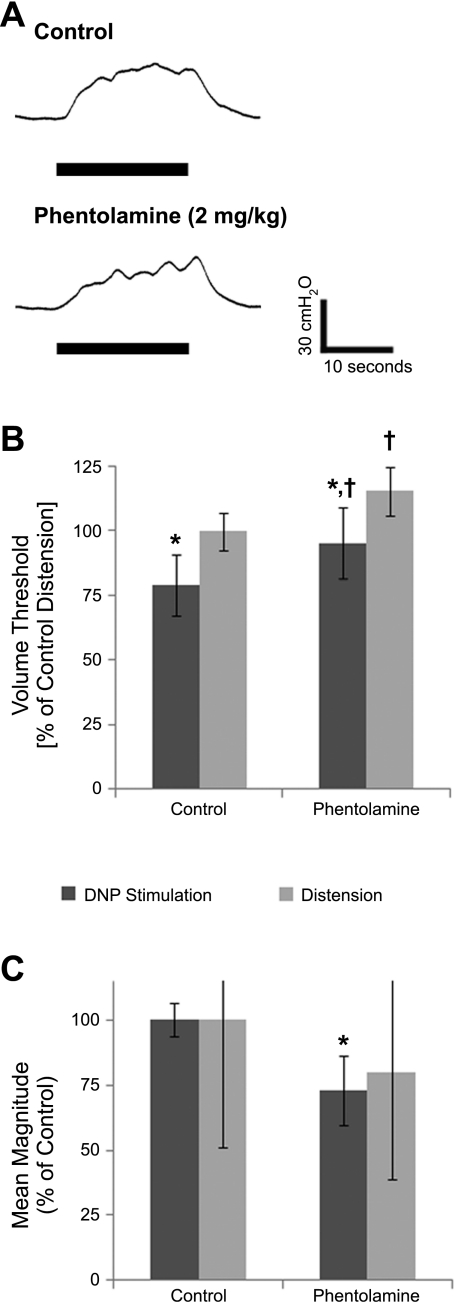
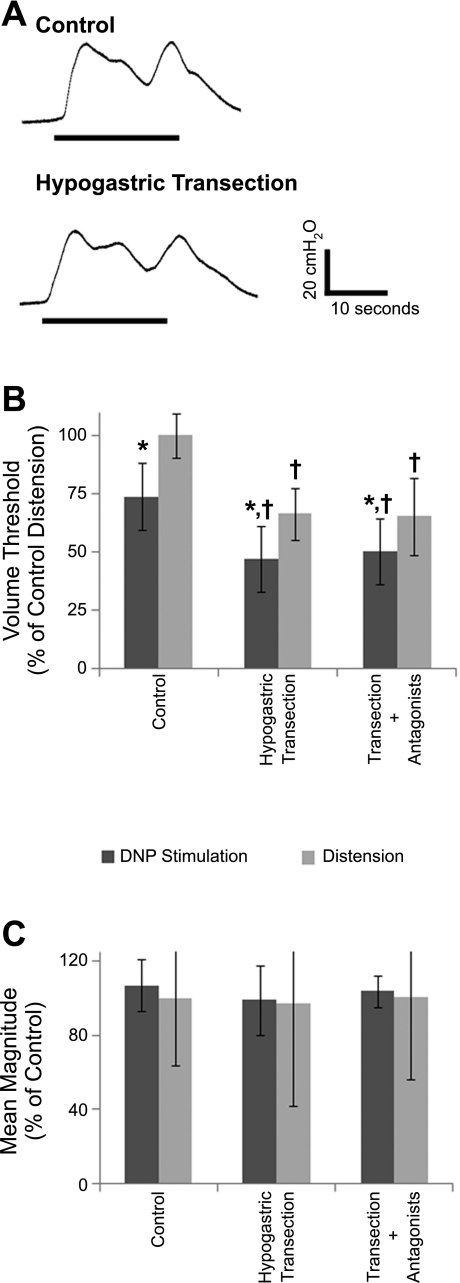
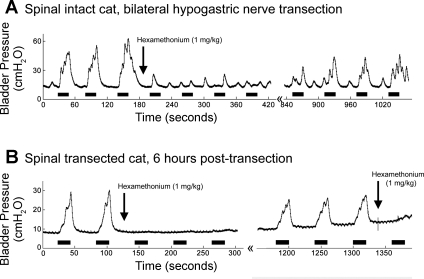
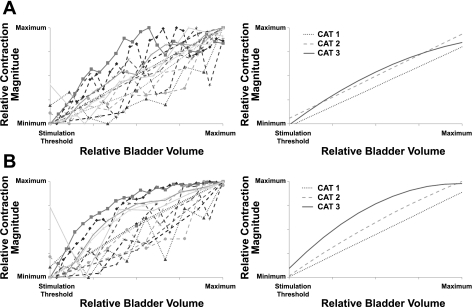
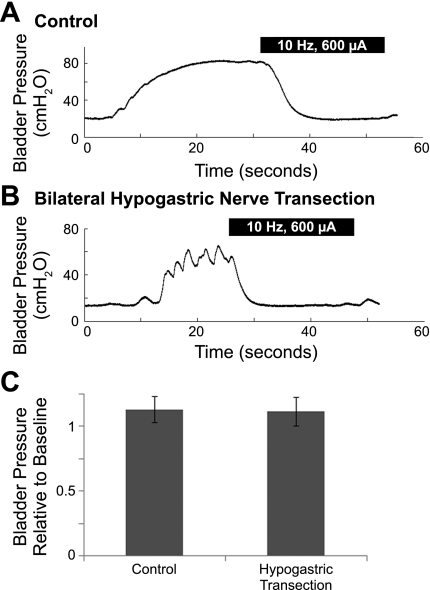
Activation of pudendal afferents can evoke bladder contraction or relaxation dependent on the frequency of stimulation, but the mechanisms of reflex bladder excitation evoked by pudendal afferent stimulation are unknown. The objective of this study was to determine the contributions of sympathetic and parasympathetic mechanisms to bladder contractions evoked by stimulation of the dorsal nerve of the penis (DNP) in α-chloralose anesthetized adult male cats. Bladder contractions were evoked by DNP stimulation only above a bladder volume threshold equal to 73 ± 12% of the distension-evoked reflex contraction volume threshold. Bilateral hypogastric nerve transection (to eliminate sympathetic innervation of the bladder) or administration of propranolol (a β-adrenergic antagonist) decreased the stimulation-evoked and distension-evoked volume thresholds by -25% to -39%. Neither hypogastric nerve transection nor propranolol affected contraction magnitude, and robust bladder contractions were still evoked by stimulation at volume thresholds below the distension-evoked volume threshold. As well, inhibition of distention-evoked reflex bladder contractions by 10 Hz stimulation of the DNP was preserved following bilateral hypogastric nerve transection. Administration of phentolamine (an α-adrenergic antagonist) increased stimulation-evoked and distension-evoked volume thresholds by 18%, but again, robust contractions were still evoked by stimulation at volumes below the distension-evoked threshold. These results indicate that sympathetic mechanisms contribute to establishing the volume dependence of reflex contractions but are not critical to the excitatory pudendal to bladder reflex. A strong correlation between the magnitude of stimulation-evoked bladder contractions and bladder volume supports that convergence of pelvic afferents and pudendal afferents is responsible for bladder excitation evoked by pudendal afferents. Further, abolition of stimulation-evoked bladder contractions following administration of hexamethonium bromide confirmed that contractions were generated by pelvic efferent activation via the pelvic ganglion. These findings indicate that pudendal afferent stimulation evokes bladder contractions through convergence with pelvic afferents to increase pelvic efferent activity.
Figures
Similar articles
-
Bladder activation by selective stimulation of pudendal nerve afferents in the cat.Exp Neurol. 2008 Jul;212(1):218-25. doi: 10.1016/j.expneurol.2008.04.010. Epub 2008 Apr 20. Exp Neurol. 2008. PMID: 18502417 Free PMC article.
-
Intraurethral stimulation evokes bladder responses via 2 distinct reflex pathways.J Urol. 2009 Jul;182(1):366-73. doi: 10.1016/j.juro.2009.02.110. Epub 2009 May 17. J Urol. 2009. PMID: 19447414 Free PMC article.
-
Activation and inhibition of the micturition reflex by penile afferents in the cat.Am J Physiol Regul Integr Comp Physiol. 2008 Jun;294(6):R1880-9. doi: 10.1152/ajpregu.00029.2008. Epub 2008 Apr 23. Am J Physiol Regul Integr Comp Physiol. 2008. PMID: 18434446 Free PMC article.
-
Integrative control of the lower urinary tract: preclinical perspective.Br J Pharmacol. 2006 Feb;147 Suppl 2(Suppl 2):S25-40. doi: 10.1038/sj.bjp.0706604. Br J Pharmacol. 2006. PMID: 16465182 Free PMC article. Review.
-
Serotonergic modulation of bladder afferent pathways.Urology. 2003 Oct;62(4 Suppl 1):10-5. doi: 10.1016/s0090-4295(03)00590-9. Urology. 2003. PMID: 14550832 Review.
Cited by
-
Modeling the spinal pudendo-vesical reflex for bladder control by pudendal afferent stimulation.J Comput Neurosci. 2016 Jun;40(3):283-96. doi: 10.1007/s10827-016-0597-5. Epub 2016 Mar 11. J Comput Neurosci. 2016. PMID: 26968615 Free PMC article.
-
High-density spinal cord stimulation selectively activates lower urinary tract nerves.J Neural Eng. 2022 Nov 22;19(6):066014. doi: 10.1088/1741-2552/aca0c2. J Neural Eng. 2022. PMID: 36343359 Free PMC article.
-
Model-based analysis of the acute effects of transcutaneous magnetic spinal cord stimulation on micturition after spinal cord injury in humans.PLoS Comput Biol. 2024 Jul 1;20(7):e1012237. doi: 10.1371/journal.pcbi.1012237. eCollection 2024 Jul. PLoS Comput Biol. 2024. PMID: 38950067 Free PMC article.
-
Electrical stimulation for the treatment of lower urinary tract dysfunction after spinal cord injury.J Spinal Cord Med. 2015 Mar;38(2):135-46. doi: 10.1179/2045772314Y.0000000299. Epub 2015 Jan 13. J Spinal Cord Med. 2015. PMID: 25582564 Free PMC article. Review.
-
Laparoscopic selective pudendal neuromodulation for neurogenic bladder: a review of literature.Cent European J Urol. 2020;73(1):39-41. doi: 10.5173/ceju.2020.0036. Epub 2020 Mar 23. Cent European J Urol. 2020. PMID: 32395321 Free PMC article.
References
-
- Andersson KE. Pharmacology of lower urinary tract smooth muscles and penile erectile tissues. Pharm Rev 45:254–308, 1993 - PubMed
-
- Andersson KE. α1-Adrenoceptors and bladder function. Eur Urol 36,Suppl 1:96–102, 1999 - PubMed
-
- Barrington FJF. The component reflexes of micturition in the cat, parts I and II. Brain 54:177–188, 1931
-
- Boggs JW, Wenzel BJ, Gustafson KJ, Grill WM. Spinal micturition reflex mediated by afferents in the deep perineal nerve. J Neurophysiol 93:2688–2697, 2005 - PubMed
-
- Boggs JW, Wenzel BJ, Gustafson KJ, Grill WM. Bladder emptying by intermittent electrical stimulation of the pudendal nerve. J Neural Eng 3:43–51, 2006 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous