

Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients
- PMID: 21068427
- PMCID: PMC3013585
- DOI: 10.1212/WNL.0b013e318202013a
Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients
Abstract
Objective: Motor recovery after stroke depends on the integrity of ipsilesional motor circuits and interactions between the ipsilesional and contralesional hemispheres. In this sham-controlled randomized trial, we investigated whether noninvasive modulation of regional excitability of bilateral motor cortices in combination with physical and occupational therapy improves motor outcome after stroke.
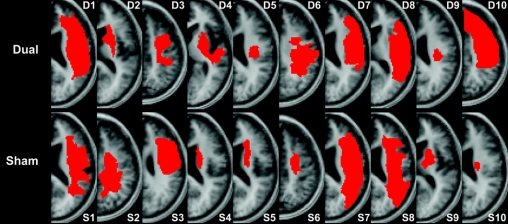
Methods: Twenty chronic stroke patients were randomly assigned to receive 5 consecutive sessions of either 1) bihemispheric transcranial direct current stimulation (tDCS) (anodal tDCS to upregulate excitability of ipsilesional motor cortex and cathodal tDCS to downregulate excitability of contralesional motor cortex) with simultaneous physical/occupational therapy or 2) sham stimulation with simultaneous physical/occupational therapy. Changes in motor impairment (Upper Extremity Fugl-Meyer) and motor activity (Wolf Motor Function Test) assessments were outcome measures while functional imaging parameters were used to identify neural correlates of motor improvement.
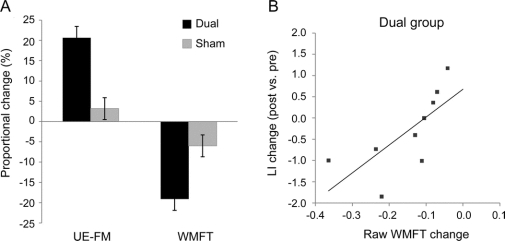
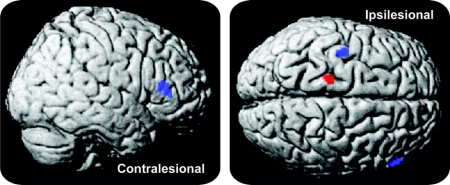
Results: The improvement of motor function was significantly greater in the real stimulation group (20.7% in Fugl-Meyer and 19.1% in Wolf Motor Function Test scores) when compared to the sham group (3.2% in Fugl-Meyer and 6.0% in Wolf Motor Function Test scores). The effects outlasted the stimulation by at least 1 week. In the real-stimulation group, stronger activation of intact ipsilesional motor regions during paced movements of the affected limb were found postintervention whereas no significant activation changes were seen in the control group.
Conclusions: The combination of bihemispheric tDCS and peripheral sensorimotor activities improved motor functions in chronic stroke patients that outlasted the intervention period. This novel approach may potentiate cerebral adaptive processes that facilitate motor recovery after stroke.
Classification of evidence: This study provides Class I evidence that for adult patients with ischemic stroke treated at least 5 months after their first and only stroke, bihemispheric tDCS and simultaneous physical/occupational therapy given over 5 consecutive sessions significantly improves motor function as measured by the Upper Extremity Fugl-Meyer assessment (raw change treated 6.1 ± 3.4, sham 1.2 ± 1.0).
Figures
Comment in
-
Influencing poststroke plasticity with electromagnetic brain stimulation: myth or reality?Neurology. 2010 Dec 14;75(24):2146-7. doi: 10.1212/WNL.0b013e31820204d9. Epub 2010 Nov 10. Neurology. 2010. PMID: 21068425 No abstract available.
References
-
- Clarke PJ, Black SE, Badley EM, Lawrence JM, Williams JI. Handicap in stroke survivors. Disabil Rehabil 1999;21:116–123. - PubMed
-
- Cramer SC. Repairing the human brain after stroke: II: restorative therapies. Ann Neurol 2008;63:549–560. - PubMed
-
- Ziemann U. Improving disability in stroke with RTMS. Lancet Neurol 2005;4:454–455. - PubMed
-
- Murase N, Duque J, Mazzocchio R, Cohen LG. Influence of interhemispheric interactions on motor function in chronic stroke. Ann Neurol 2004;55:400–409. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials