

Comparing gray mineral trioxide aggregate and diluted formocresol in pulpotomized human primary molars
- PMID: 21070705
- PMCID: PMC4889336
Comparing gray mineral trioxide aggregate and diluted formocresol in pulpotomized human primary molars
Abstract
Purpose: The purpose of this multisite, multioperator, prospective, randomized, controlled clinical trial was to evaluate the 6-month outcomes of diluted formocresol (DFC) compared to gray mineral trioxide aggregate (GMTA) as pulpotomy medicament.
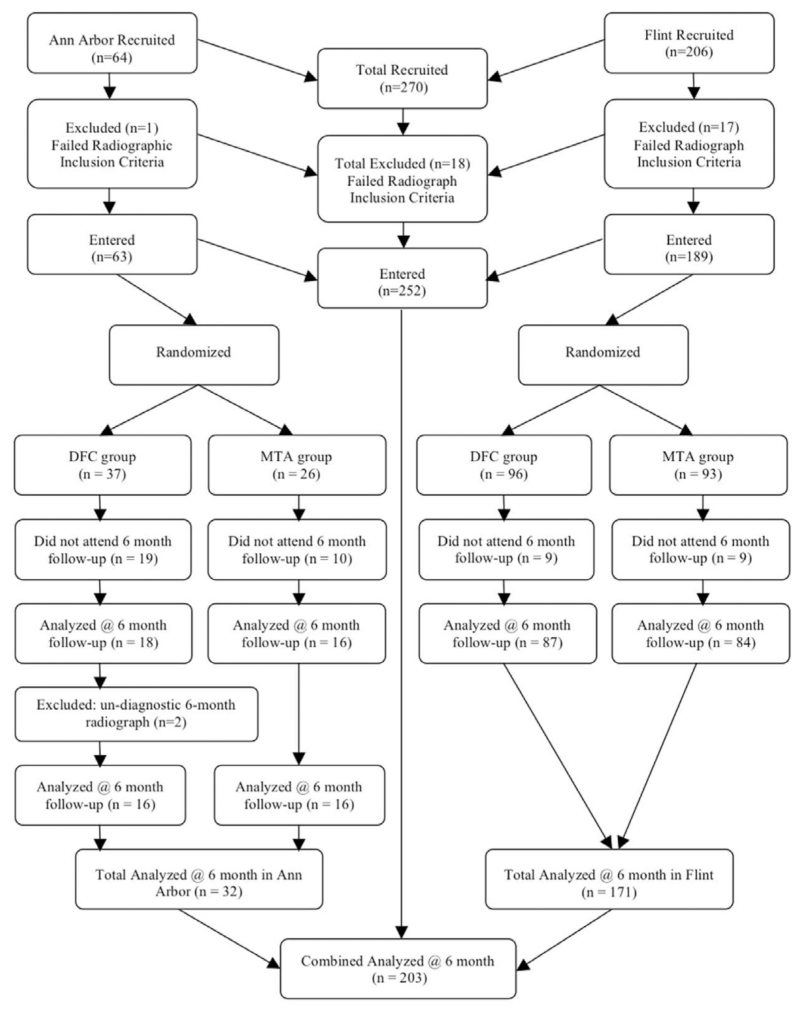
Methods: Determined by a power analysis, 252 molars of 152 children were recruited. The teeth were randomly assigned to receive GMTA or DFC. At the 6-month follow-up, 118 children with 203 treated teeth were evaluated.
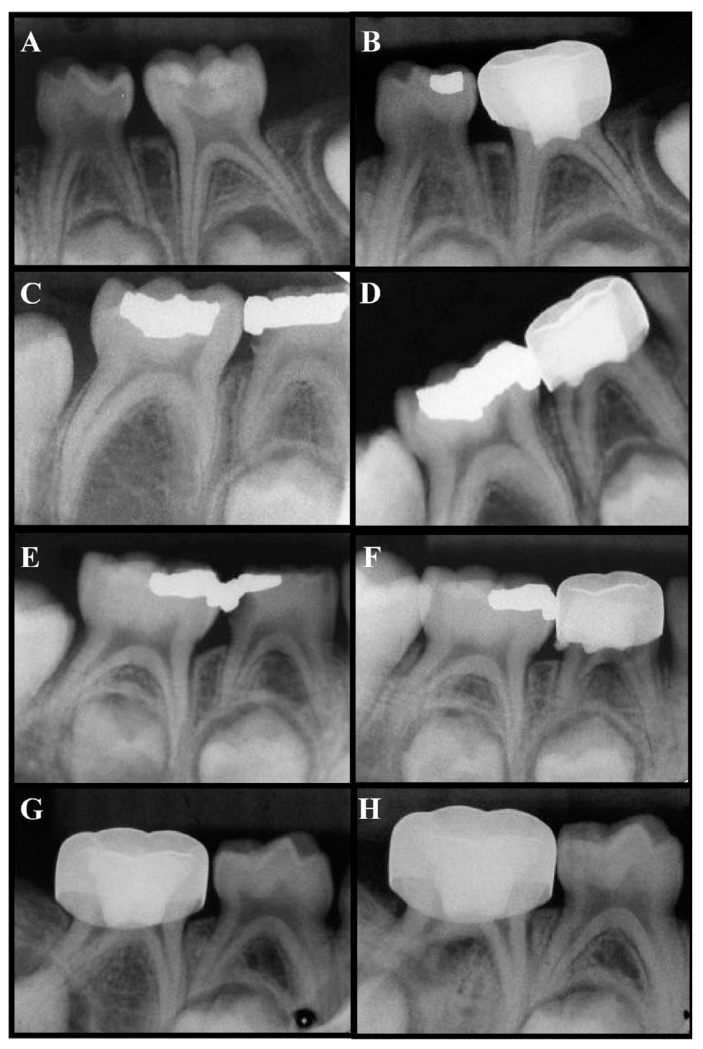
Results: Four blinded and calibrated evaluators scored each radiograph for pathologies. Clinical success was similar for DFC (97%) and GMTA (100%), (P<.09). Radiographic success differed significantly (P<.04) for DFC (86%) and GMTA (95%). Pulp canal obliteration was radiographically observed in 25% of the DFC group and in 37% of the GMTA group (P=.07). Dentin bridging was observed in 22% of the GMTA group but was not found in the DFC group (P<.01).
Conclusion: Teeth treated with GMTA showed more favorable radiographic outcomes than DFC at 6 months post-treatment.
Figures
References
-
- Seale NS, Glickman GN. Contemporary perspectives on vital pulp therapy: Views from the endodontists and pediatric dentists. Pediatr Dent. 2008;30:261–7. - PubMed
-
- Milnes AR. Is formocresol obsolete? A fresh look at the evidence concerning safety issues. Pediatr Dent. 2008;30:237–46. - PubMed
-
- Fuks AB, Papagiannoulis L. Pulpotomy in primary teeth: Review of the literature according to standardized criteria. Eur Arch Paediatr Dent. 2006;7:64–71. discussion 72. - PubMed
-
- American Academy of Pediatric Dentistry Clinical Affairs Committee Guideline on pulp therapy for primary and young permanent teeth. Pediatr Dent. 2008;29:163–7.
-
- Casas MJ, Kenny DJ, Judd PL, Johnston DH. Do we still need formocresol in pediatric dentistry? J Can Dent Assoc. 2005;71:749–51. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
