

Assessment of conventional cardiovascular risk factors and multiple biomarkers for the prediction of incident heart failure and atrial fibrillation
- PMID: 21070922
- PMCID: PMC3005324
- DOI: 10.1016/j.jacc.2010.05.049
Assessment of conventional cardiovascular risk factors and multiple biomarkers for the prediction of incident heart failure and atrial fibrillation
Abstract
Objectives: the purpose of this study was to assess the predictive accuracy of conventional cardiovascular risk factors for incident heart failure and atrial fibrillation, and the added benefit of multiple biomarkers reflecting diverse pathophysiological pathways.
Background: heart failure and atrial fibrillation are interrelated cardiac diseases associated with substantial morbidity and mortality and increasing incidence. Data on prediction and prevention of these diseases in healthy individuals are limited.
Methods: in 5,187 individuals from the community-based MDCS (Malmö Diet and Cancer Study), we studied the performance of conventional risk factors and 6 biomarkers including midregional pro-atrial natriuretic peptide (MR-proANP), N-terminal pro-B-type natriuretic peptide (NT-proBNP), midregional pro-adrenomedullin, cystatin C, C-reactive protein (CRP), and copeptin.
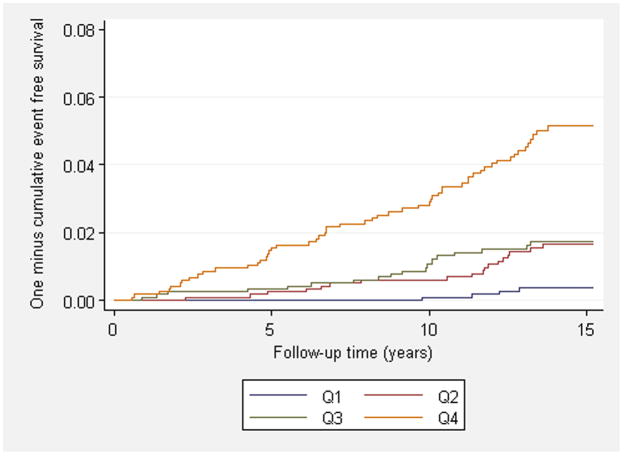
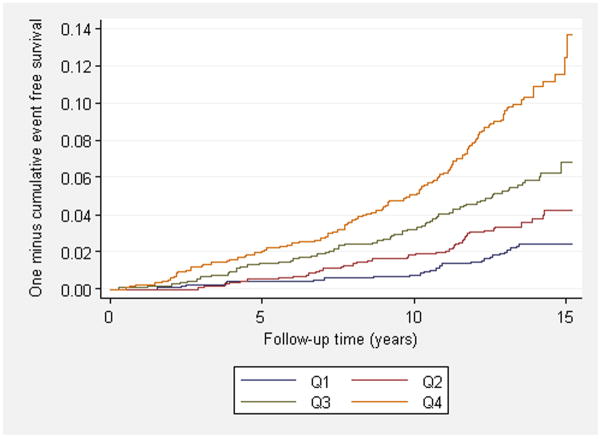
Results: during a mean follow-up of 14 years, 112 individuals were diagnosed with heart failure and 284 individuals with atrial fibrillation. NT-proBNP (hazard ratio [HR]: 1.63 per SD, 95% confidence interval [CI]: 1.29 to 2.06, p < 0.001), CRP (HR: 1.57 per SD, 95% CI: 1.28 to 1.94, p < 0.001), and MR-proANP (HR: 1.26 per SD, 95% CI: 1.02 to 1.56, p = 0.03) predicted incident heart failure independently of conventional risk factors and other biomarkers. MR-proANP (HR: 1.62, 95% CI: 1.42 to 1.84, p < 0.001) and CRP (HR: 1.18, 95% CI: 1.03 to 1.34, p = 0.01) independently predicted atrial fibrillation. Addition of biomarkers to conventional risk factors improved c-statistics from 0.815 to 0.842 for heart failure and from 0.732 to 0.753 for atrial fibrillation and the integrated discrimination improvement for both diseases (p < 0.001). Net reclassification improvement (NRI) with biomarkers was observed in 22% of individuals for heart failure (NRI, p < 0.001) and in 7% for atrial fibrillation (NRI, p = 0.06), mainly due to up-classification of individuals who developed disease (heart failure: 29%, atrial fibrillation: 19%). Addition of CRP to natriuretic peptides did not improve discrimination or reclassification.
Conclusions: conventional cardiovascular risk factors predict incident heart failure and atrial fibrillation with reasonable accuracy in middle-age individuals free from disease. Natriuretic peptides, but not other biomarkers, improve discrimination modestly for both diseases above and beyond conventional risk factors and substantially improve risk classification for heart failure.
2010 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Joachim Struck, Nils G. Morgenthaler and Andreas Bergmann are employees of Brahms AG, which holds patent rights on the assays used for MR-proADM, MR-proANP and Copeptin.
Figures
References
-
- Braunwald E. Shattuck lecture--cardiovascular medicine at the turn of the millennium: triumphs, concerns, and opportunities. N Engl J Med. 1997;337:1360–1369. - PubMed
-
- Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol. 2003;91 (suppl):2D–8D. - PubMed
-
- Roger VL, Weston SA, Redfield MM, et al. Trends in heart failure incidence and survival in a community-based population. JAMA. 2004;292:344–350. - PubMed
-
- Stewart S, Hart CL, Hole DJ, McMurray JJV. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the renfrew/paisley study. Am J Med. 2002;113:359–364. - PubMed
-
- Lloyd-Jones DM, Larson MG, Leip EP, et al. Lifetime risk for developing congestive heart failure: the Framingham heart study. Circulation. 2002;106:3068–3072. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
