

Prognostic factors for intensive care unit admission, intensive care outcome, and post-intensive care survival in patients with de novo acute myeloid leukemia: a single center experience
- PMID: 21071501
- PMCID: PMC3031690
- DOI: 10.3324/haematol.2010.031583
Prognostic factors for intensive care unit admission, intensive care outcome, and post-intensive care survival in patients with de novo acute myeloid leukemia: a single center experience
Abstract
Background: Acute myeloid leukemia is a life-threatening disease associated with high mortality rates. A substantial number of patients require intensive care. This investigation analyzes risk factors predicting admission to the intensive care unit in patients with acute myeloid leukemia eligible for induction chemotherapy, the outcome of these patients, and prognostic factors predicting their survival.
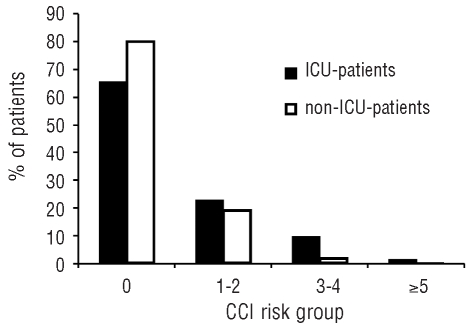
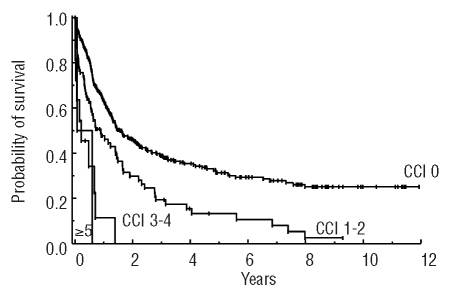
Design and methods: A total of 406 consecutive patients with de novo acute myeloid leukemia (15-89 years) were analyzed retrospectively. Markers recorded at the time of diagnosis included karyotype, fibrinogen, C-reactive protein, and Charlson comorbidity index. In patients requiring critical care, the value of the Simplified Acute Physiology Score II, the need for mechanical ventilation, and vasopressor support were recorded at the time of intensive care unit admission. The independent prognostic relevance of the parameters was tested by multivariate analysis.
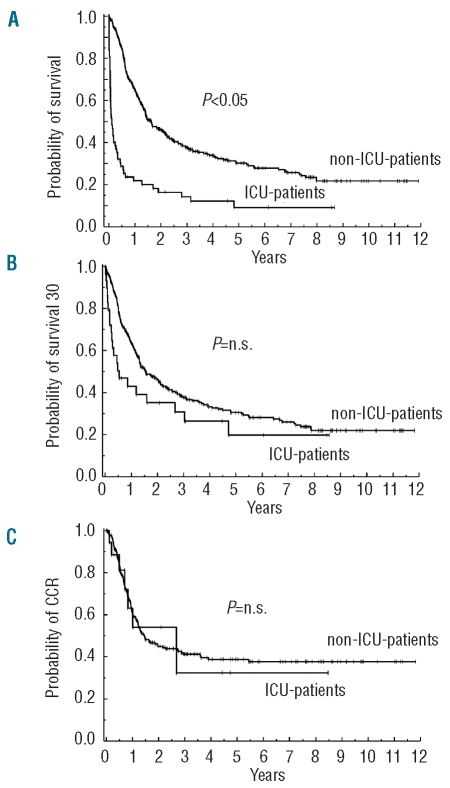
Results: Sixty-two patients (15.3%) required intensive care, primarily due to respiratory failure (50.0%) or life-threatening bleeding (22.6%). Independent risk factors predicting intensive care unit admission were lower fibrinogen concentration, the presence of an infection, and comorbidity. The survival rate was 45%, with the Simplified Acute Physiology Score II being the only independent prognostic parameter (P<0.05). Survival was inferior in intensive care patients compared to patients not admitted to an intensive care unit. However, no difference between intensive care and non-intensive care patients was found concerning continuous complete remission at 6 years or survival at 6 years in patients who survived the first 30 days after diagnosis (non-intensive care patients: 28%; intensive care patients: 20%, P>0.05).
Conclusions: Ongoing infections, low fibrinogen and comorbidity are predictive for intensive care unit admission in acute myeloid leukemia. Although admission was a risk factor for survival, continuous complete remission and survival of patients alive at day 30 were similar in patients who were admitted or not admitted to an intensive care unit.
Figures
References
-
- Stone RM, O’Donnell MR, Sekeres MA. Acute myeloid leukemia. Hematology Am Soc Hematol Educ Program. 2004:98–117. - PubMed
-
- Vellenga E, Griffin JD. The biology of acute myeloblastic leukemia. Semin Oncol. 1987;14(4):365–71. - PubMed
-
- Grimwade D, Walker H, Oliver F, Wheatley K, Harrison C, Harrison G, et al. The importance of diagnostic cytogenetics on outcome in AML: analysis of 1,612 patients entered into the MRC AML 10 trial. The Medical Research Council Adult and Children’s Leukaemia Working Parties. Blood. 1998;92(7):2322–33. - PubMed
-
- Grimwade D, Walker H, Harrison G, Oliver F, Chatters S, Harrison CJ, et al. The predictive value of hierarchical cytogenetic classification in older adults with acute myeloid leukemia (AML): analysis of 1065 patients entered into the United Kingdom Medical Research Council AML11 trial. Blood. 2001;98(5):1312–20. - PubMed
-
- Strout MP, Marcucci G, Caligiuri MA, Bloomfield CD. Core-binding factor (CBF) and MLL-associated primary acute myeloid leukemia: biology and clinical implications. Ann Hematol. 1999;78(6):251–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
