

A migration signature and plasma biomarker panel for pancreatic adenocarcinoma
- PMID: 21071578
- PMCID: PMC3635082
- DOI: 10.1158/1940-6207.CAPR-10-0025
A migration signature and plasma biomarker panel for pancreatic adenocarcinoma
Abstract
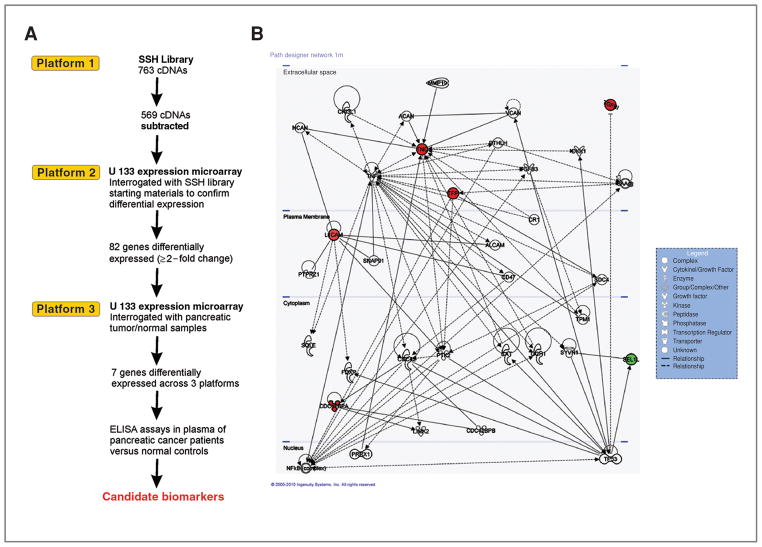
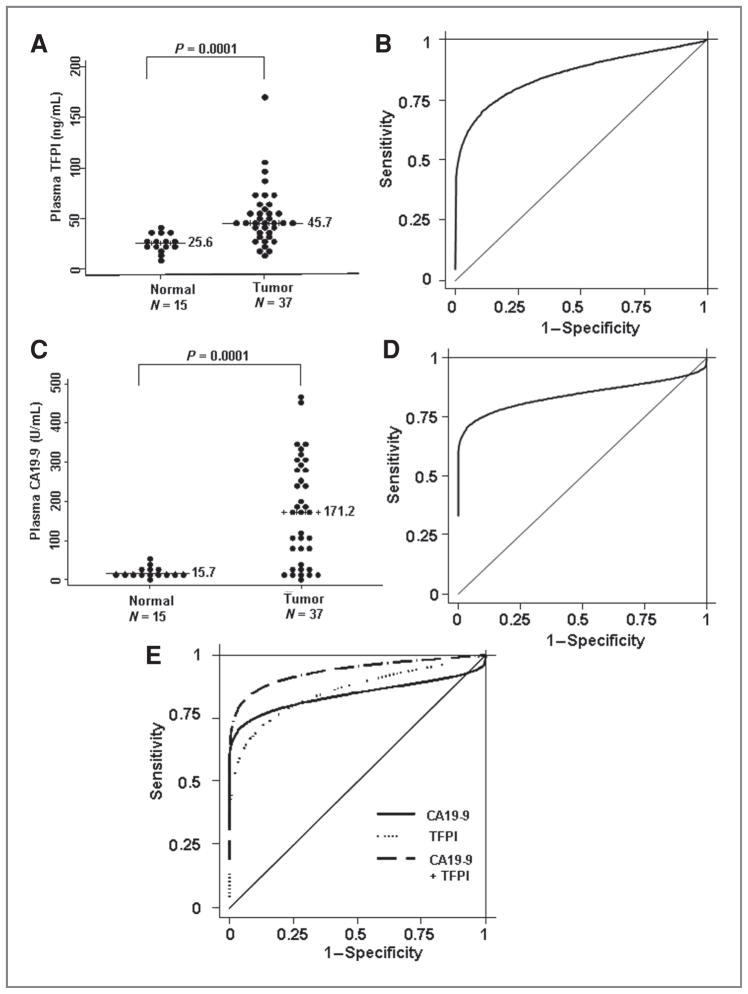
Pancreatic ductal adenocarcinoma is a disease of extremely poor prognosis for which there are no reliable markers of asymptomatic disease. To identify pancreatic cancer biomarkers, we focused on a genomic interval proximal to the most common fragile site in the human genome, chromosome 3p12, which undergoes smoking-related breakage, loss of heterozygosity, and homozygous deletion as an early event in many epithelial tumors, including pancreatic cancers. Using a functional genomic approach, we identified a seven-gene panel (TNC, TFPI, TGFBI, SEL-1L, L1CAM, WWTR1, and CDC42BPA) that was differentially expressed across three different expression platforms, including pancreatic tumor/normal samples. In addition, Ingenuity Pathways Analysis (IPA) and literature searches indicated that this seven-gene panel functions in one network associated with cellular movement/morphology/development, indicative of a "migration signature" of the 3p pathway. We tested whether two secreted proteins from this panel, tenascin C (TNC) and tissue factor pathway inhibitor (TFPI), could serve as plasma biomarkers. Plasma ELISA assays for TFPI/TNC resulted in a combined area under the curve (AUC) of 0.88 and, with addition of CA19-9, a combined AUC for the three-gene panel (TNC/TFPI/CA19-9), of 0.99 with 100% specificity at 90% sensitivity and 97.22% sensitivity at 90% specificity. Validation studies using TFPI only in a blinded sample set increased the performance of CA19-9 from an AUC of 0.84 to 0.94 with the two-gene panel. Results identify a novel 3p pathway-associated migration signature and plasma biomarker panel that has utility for discrimination of pancreatic cancer from normal controls and promise for clinical application.
©2010 AACR.
Conflict of interest statement
No potential conflicts of interest were disclosed.
Figures

References
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer Statistics, 2009. CACancer J Clin. 2009;59:225–49. - PubMed
-
- Kim HR, Lee CH, Kim YW, Han SK, Shim YS, Yim JJ. Increased CA 19–9 level in patients without malignant disease. Clin Chem Lab Med. 2009;47:750–4. - PubMed
-
- Stein CK, Glover TW, Palmer JL, Glisson BS. Direct correlation between FRA3B expression and cigarette smoking. Genes Chromosomes Cancer. 2002;34:333–40. - PubMed
-
- Shridhar R, Shridhar V, Wang X, Paradee W, Dugan M, Sarkar F, et al. Frequent breakpoints in the 3p14. 2 fragile site, FRA3B, in pancreatic tumors. Cancer Res. 1996;56:4347–50. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
