

Neurogenic thoracic outlet syndrome: A case report and review of the literature
- PMID: 21072145
- PMCID: PMC2966747
- DOI: 10.4103/0973-6042.70817
Neurogenic thoracic outlet syndrome: A case report and review of the literature
Abstract
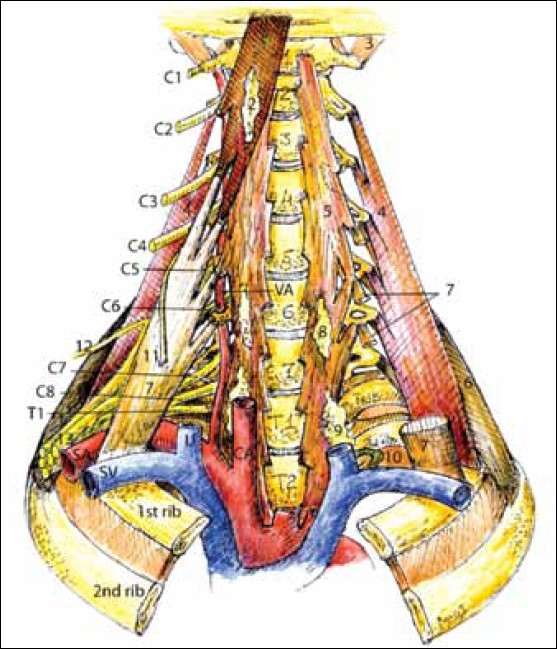
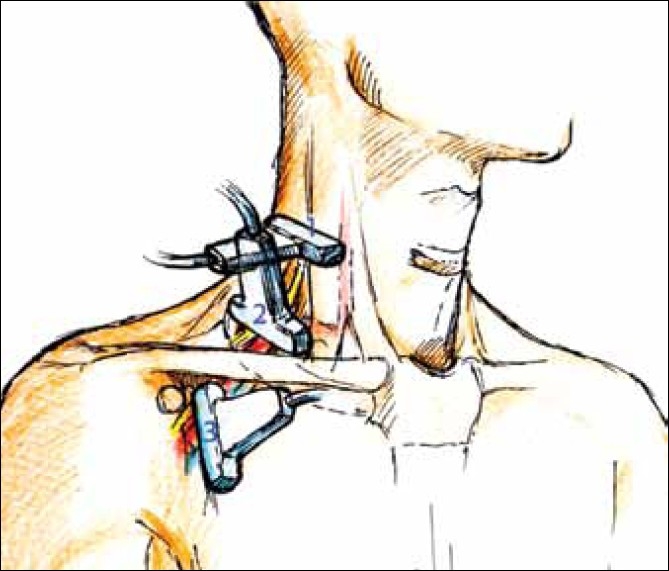
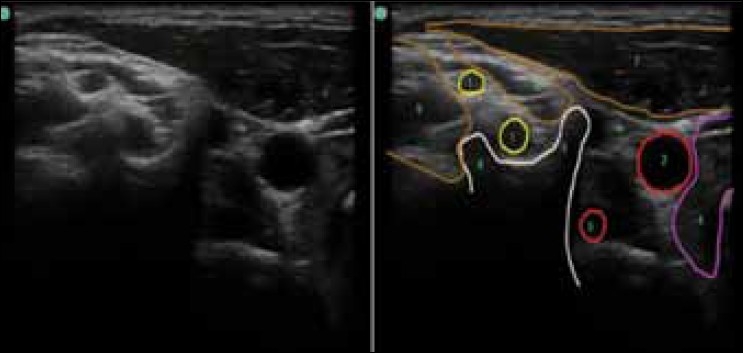
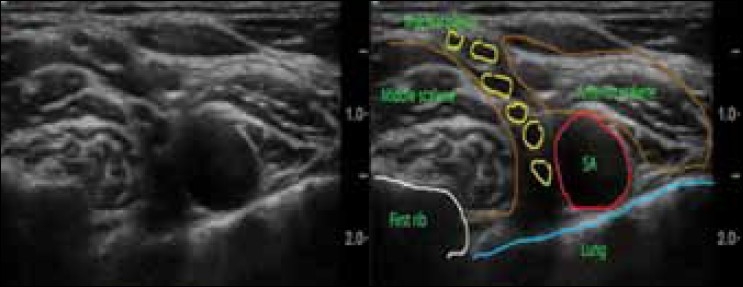
Neurogenic thoracic outlet syndrome (NTOS) is an oft-overlooked and obscure cause of shoulder pain, which regularly presents to the office of shoulder surgeons and pain specialist. With this paper we present an otherwise healthy young female patient with typical NTOS. She first received repeated conservative treatments with 60 units of botulinium toxin injected into the anterior scalene muscle at three-month intervals, which providing excellent results of symptom-free periods. Later a trans-axillary first rib resection provided semi-permanent relief. The patient was followed for 10 years after which time the symptoms reappeared. We review the literature and elaborate on the anatomy, sonoanatomy, etiology and characteristics, symptoms, diagnostic criteria and treatment modalities of NTOS. Patients with NTOS often get operated upon - even if just a diagnostic arthroscopy, and an interscalene or other brachial plexus block may be performed. This might put the patient in jeopardy of permanent nerve injury, and the purpose of this review is to minimize or prevent this.
Keywords: Acute pain; botox; neurogenic thoracic outlet syndrome; shoulder pain; thoracic outlet syndrome.
Conflict of interest statement
Figures
Similar articles
-
Recurrent neurogenic thoracic outlet syndrome.Am J Surg. 2004 Apr;187(4):505-10. doi: 10.1016/j.amjsurg.2003.12.050. Am J Surg. 2004. PMID: 15041500
-
Redo surgery for neurogenic thoracic outlet syndrome is useful.J Vasc Surg. 2022 Aug;76(2):531-537.e1. doi: 10.1016/j.jvs.2022.03.863. Epub 2022 Mar 31. J Vasc Surg. 2022. PMID: 35367561
-
Rib-sparing scalenectomy for neurogenic thoracic outlet syndrome: Early results.J Vasc Surg. 2021 Jun;73(6):2059-2063. doi: 10.1016/j.jvs.2020.12.052. Epub 2020 Dec 17. J Vasc Surg. 2021. PMID: 33340695
-
Challenges and Advances in the Diagnosis and Management of Neurogenic Thoracic Outlet Syndrome: A Comprehensive Review.J Hand Surg Asian Pac Vol. 2024 Aug;29(4):269-280. doi: 10.1142/S2424835524400010. Epub 2024 Jul 26. J Hand Surg Asian Pac Vol. 2024. PMID: 39051151 Review.
-
Neurogenic thoracic outlet syndrome in the overhead and throwing athlete: A narrative review.PM R. 2023 May;15(5):629-639. doi: 10.1002/pmrj.12816. Epub 2022 Jun 13. PM R. 2023. PMID: 35403345 Review.
Cited by
-
A Cadaveric Investigation of the Dorsal Scapular Nerve.Anat Res Int. 2016;2016:4106981. doi: 10.1155/2016/4106981. Epub 2016 Aug 15. Anat Res Int. 2016. PMID: 27597900 Free PMC article.
-
Evaluation of Complications after Surgical Treatment of Thoracic Outlet Syndrome.Korean J Thorac Cardiovasc Surg. 2017 Feb;50(1):36-40. doi: 10.5090/kjtcs.2017.50.1.36. Epub 2017 Feb 5. Korean J Thorac Cardiovasc Surg. 2017. PMID: 28180101 Free PMC article.
-
Arm Numbness at 45 Degrees Abduction: A Case Report of Thoracic Outlet Syndrome After Brachial Neuritis.J Rehabil Med Clin Commun. 2020 Jun 15;3:1000034. doi: 10.2340/20030711-1000034. eCollection 2020. J Rehabil Med Clin Commun. 2020. PMID: 33884136 Free PMC article.
-
Pectoralis minor syndrome: diagnosis with Botulinum injection and treatment with tenotomy - a prospective case series.Shoulder Elbow. 2022 Apr;14(2):157-161. doi: 10.1177/1758573220968454. Epub 2020 Oct 25. Shoulder Elbow. 2022. PMID: 35265181 Free PMC article.
-
Concomitant neurogenic and vascular thoracic outlet syndrome due to multiple exostoses.Ann Card Anaesth. 2018 Jan-Mar;21(1):71-73. doi: 10.4103/aca.ACA_119_17. Ann Card Anaesth. 2018. PMID: 29336398 Free PMC article.
References
-
- Watson LA, Pizzari T, Balster S. Thoracic outlet syndrome part 1: Clinical manifestations, differentiation and treatment pathways. Man Ther. 2009;14:586–95. - PubMed
-
- Thomas GI, Jones TW, Stavney LS, Manhas DR. The middle scalene muscle and its contribution to the TOC. Am J Surg. 1983;145:589–92. - PubMed
-
- Roos DB. Historical perspectives and anatomic considerations. Thoracic outlet syndrome. Semin Thorac Cardiovasc Surg. 1996;8:183–9. - PubMed
-
- Nichols AW. Diagnosis and management of thoracic outlet syndrome. Curr Sports Med Rep. 2009;8:240–9. - PubMed
LinkOut - more resources
Full Text Sources
