

The impact of case diagnosis coverage and diagnosis delays on the effectiveness of antiviral strategies in mitigating pandemic influenza A/H1N1 2009
- PMID: 21072188
- PMCID: PMC2972206
- DOI: 10.1371/journal.pone.0013797
The impact of case diagnosis coverage and diagnosis delays on the effectiveness of antiviral strategies in mitigating pandemic influenza A/H1N1 2009
Abstract
Background: Neuraminidase inhibitors were used to reduce the transmission of pandemic influenza A/H1N1 2009 at the early stages of the 2009/2010 pandemic. Policies for diagnosis of influenza for the purposes of antiviral intervention differed markedly between and within countries, leading to differences in the timing and scale of antiviral usage.
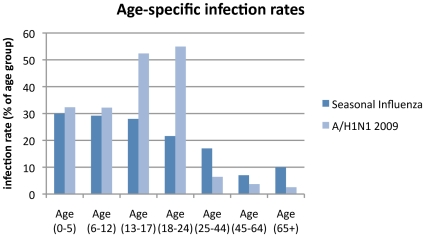
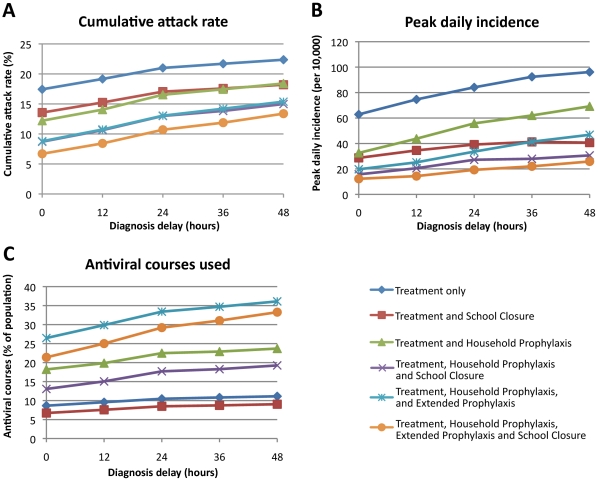
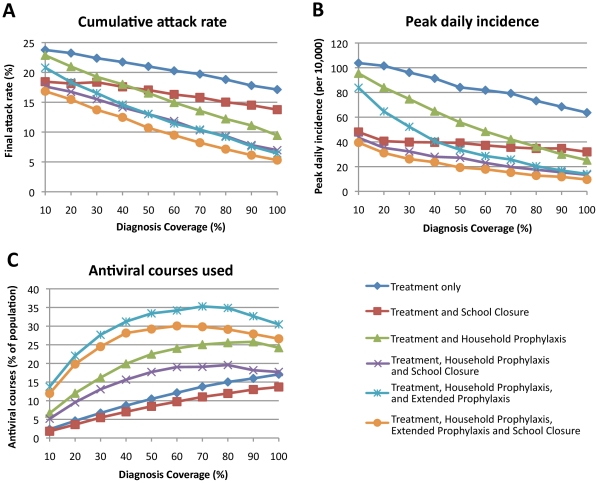
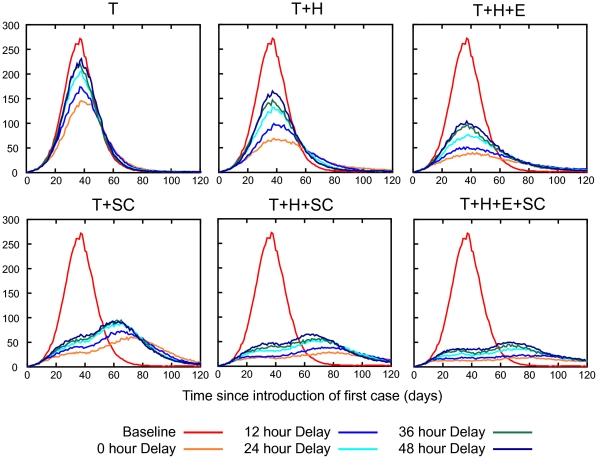
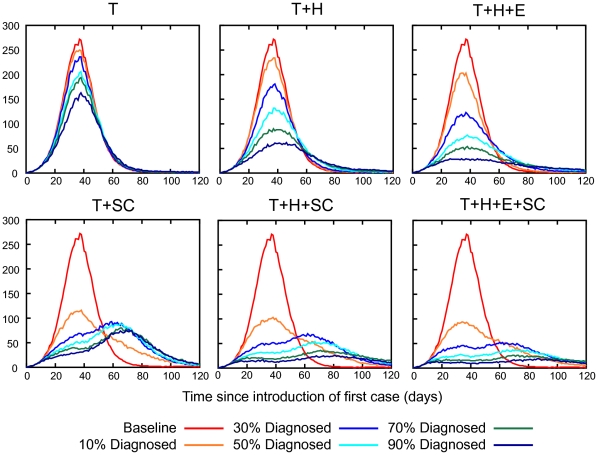
Methodology/principal findings: The impact of the percentage of symptomatic infected individuals who were diagnosed, and of delays to diagnosis, for three antiviral intervention strategies (each with and without school closure) were determined using a simulation model of an Australian community. Epidemic characteristics were based on actual data from the A/H1N1 2009 pandemic including reproduction number, serial interval and age-specific infection rate profile. In the absence of intervention an illness attack rate (AR) of 24.5% was determined from an estimated R(0) of 1.5; this was reduced to 21%, 16.5% or 13% by treatment-only, treatment plus household prophylaxis, or treatment plus household plus extended prophylaxis antiviral interventions respectively, assuming that diagnosis occurred 24 hours after symptoms arose and that 50% of symptomatic cases were diagnosed. If diagnosis occurred without delay, ARs decreased to 17%, 12.2% or 8.8% respectively. If 90% of symptomatic cases were diagnosed (with a 24 hour delay), ARs decreased to 17.8%, 11.1% and 7.6%, respectively.
Conclusion: The ability to rapidly diagnose symptomatic cases and to diagnose a high proportion of cases was shown to improve the effectiveness of all three antiviral strategies. For epidemics with R(0)< = 1.5 our results suggest that when the case diagnosis coverage exceeds ∼70% the size of the antiviral stockpile required to implement the extended prophylactic strategy decreases. The addition of at least four weeks of school closure was found to further reduce cumulative and peak attack rates and the size of the required antiviral stockpile.
Conflict of interest statement
Figures
Similar articles
-
Analysis of the effectiveness of interventions used during the 2009 A/H1N1 influenza pandemic.BMC Public Health. 2010 Mar 29;10:168. doi: 10.1186/1471-2458-10-168. BMC Public Health. 2010. PMID: 20346187 Free PMC article.
-
Secondary attack rate of pandemic influenza A(H1N1) 2009 in Western Australian households, 29 May-7 August 2009.Euro Surveill. 2011 Jan 20;16(3):19765. Euro Surveill. 2011. PMID: 21262182
-
Cost-effective strategies for mitigating a future influenza pandemic with H1N1 2009 characteristics.PLoS One. 2011;6(7):e22087. doi: 10.1371/journal.pone.0022087. Epub 2011 Jul 8. PLoS One. 2011. PMID: 21760957 Free PMC article.
-
Emerging oseltamivir resistance in seasonal and pandemic influenza A/H1N1.J Clin Virol. 2011 Oct;52(2):70-8. doi: 10.1016/j.jcv.2011.05.019. Epub 2011 Jun 17. J Clin Virol. 2011. PMID: 21684202 Review.
-
The potential for multidrug-resistant influenza.Curr Opin Infect Dis. 2011 Dec;24(6):599-604. doi: 10.1097/QCO.0b013e32834cfb43. Curr Opin Infect Dis. 2011. PMID: 22001947 Review.
Cited by
-
Efficient Vaccine Distribution Based on a Hybrid Compartmental Model.PLoS One. 2016 May 27;11(5):e0155416. doi: 10.1371/journal.pone.0155416. eCollection 2016. PLoS One. 2016. PMID: 27233015 Free PMC article.
-
Development and application of sensitive, specific, and rapid CRISPR-Cas13-based diagnosis.J Med Virol. 2021 Jul;93(7):4198-4204. doi: 10.1002/jmv.26889. Epub 2021 Mar 25. J Med Virol. 2021. PMID: 33599292 Free PMC article. Review.
-
Epidemiological consequences of household-based antiviral prophylaxis for pandemic influenza.J R Soc Interface. 2013 Feb 6;10(81):20121019. doi: 10.1098/rsif.2012.1019. Print 2013 Apr 6. J R Soc Interface. 2013. PMID: 23389899 Free PMC article.
-
Economic analysis of pandemic influenza mitigation strategies for five pandemic severity categories.BMC Public Health. 2013 Mar 8;13:211. doi: 10.1186/1471-2458-13-211. BMC Public Health. 2013. PMID: 23496898 Free PMC article.
-
A model-based economic analysis of pre-pandemic influenza vaccination cost-effectiveness.BMC Infect Dis. 2014 May 16;14:266. doi: 10.1186/1471-2334-14-266. BMC Infect Dis. 2014. PMID: 24884470 Free PMC article.
References
-
- Australian Commonwealth Department of Health and Ageing. 2009. Australian Health Management Plan for Pandemic Influenza. Available: http://www.flupandemic.gov.au/internet/panflu/publishing.nsf/Content/ahm... Accessed 11th September 2009.
-
- U.S. Department of Health and Human Services. 2009. Pandemic Influenza Plan. Available: http://www.hhs.gov/pandemicflu/plan/Accessed 11th September 2009. - PubMed
-
- United Kingdom Department of Health. 2007. Pandemic flu: A national framework for responding to an influenza pandemic. Available: http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicati...Accessed 11th September 2009.
-
- Nicoll A, Coulombier D. Europe's initial experience with pandemic (H1N1) 2009 - mitigation and delaying policies and practices. Euro Surveill. 2009;14:pii = 19279. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
