

FGFR3, HRAS, KRAS, NRAS and PIK3CA mutations in bladder cancer and their potential as biomarkers for surveillance and therapy
- PMID: 21072204
- PMCID: PMC2972209
- DOI: 10.1371/journal.pone.0013821
FGFR3, HRAS, KRAS, NRAS and PIK3CA mutations in bladder cancer and their potential as biomarkers for surveillance and therapy
Abstract
Background: Fifty percent of patients with muscle-invasive bladder cancer (MI-BC) die from their disease and current chemotherapy treatment only marginally increases survival. Novel therapies targeting receptor tyrosine kinases or activated oncogenes may improve outcome. Hence, it is necessary to stratify patients based on mutations in relevant oncogenes. Patients with non-muscle-invasive bladder cancer (NMI-BC) have excellent survival, however two-thirds develop recurrences. Tumor specific mutations can be used to detect recurrences in urine assays, presenting a more patient-friendly diagnostic procedure than cystoscopy.
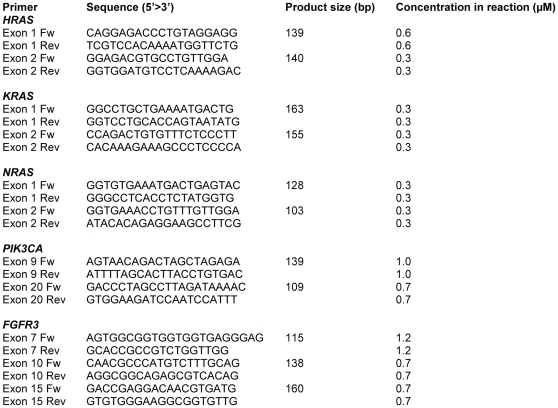
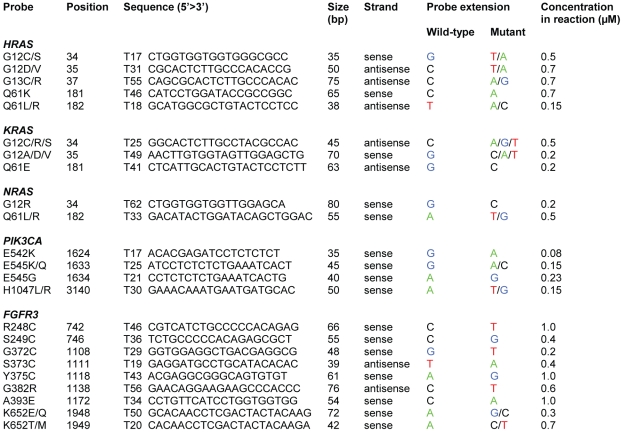
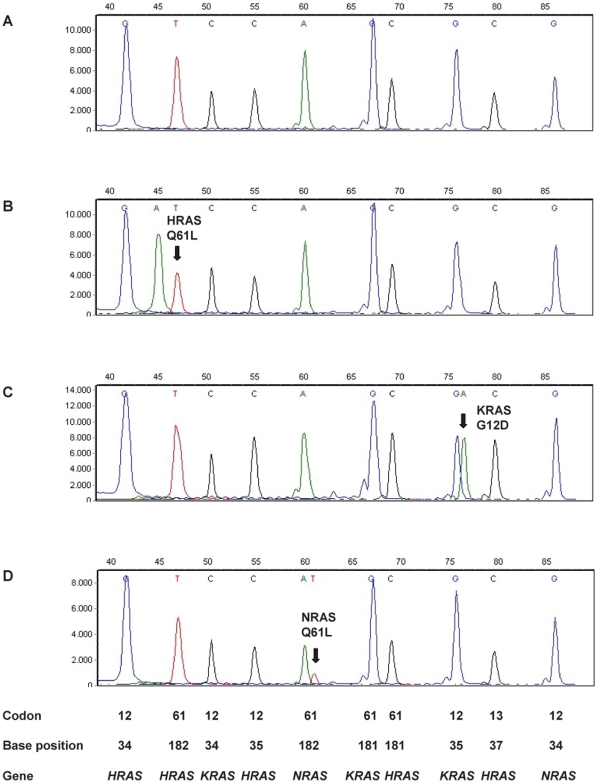
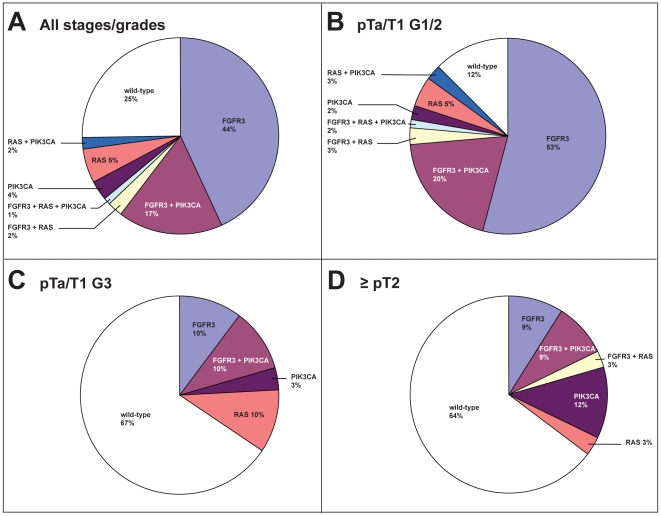
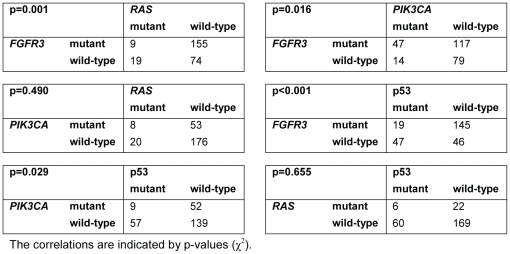
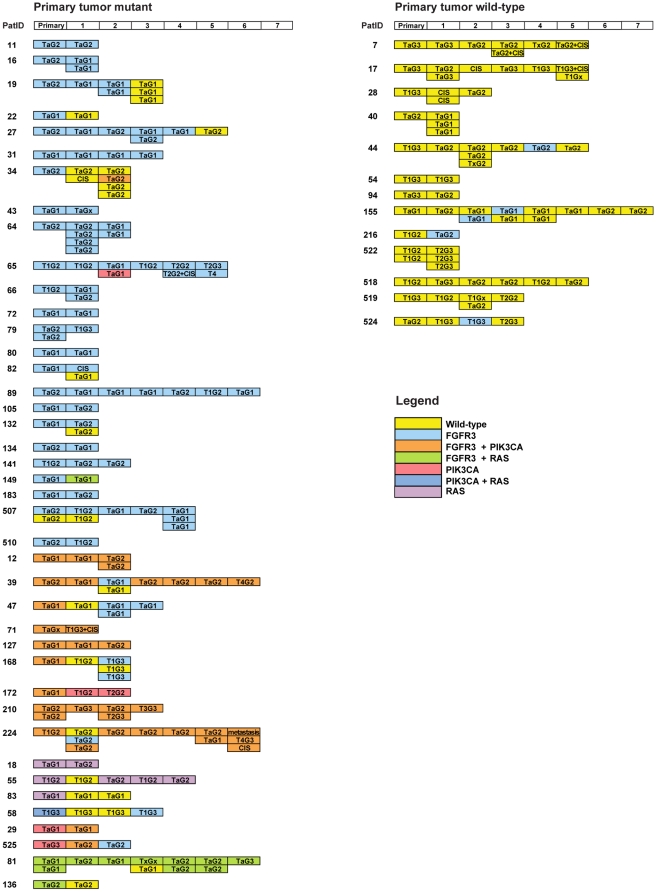
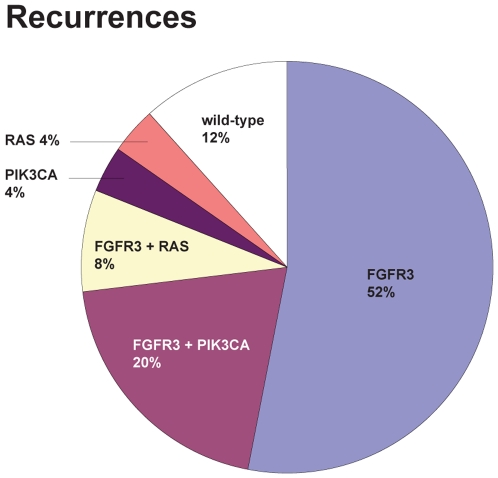
Methodology/principal findings: To address these issues, we developed a mutation assay for the simultaneous detection of 19 possible mutations in the HRAS, KRAS, and NRAS genes. With this assay and mutation assays for the FGFR3 and PIK3CA oncogenes, we screened primary bladder tumors of 257 patients and 184 recurrences from 54 patients. Additionally, in primary tumors p53 expression was obtained by immunohistochemistry. Of primary tumors 64% were mutant for FGFR3, 11% for RAS, 24% for PIK3CA, and 26% for p53. FGFR3 mutations were mutually exclusive with RAS mutations (p = 0.001) and co-occurred with PIK3CA mutations (p = 0.016). P53 overexpression was mutually exclusive with PIK3CA and FGFR3 mutations (p≤0.029). Mutations in the RAS and PIK3CA genes were not predictors for recurrence-free, progression-free and disease-specific survival. In patients presenting with NMI-BC grade 3 and MI-BC, 33 and 36% of the primary tumors were mutant. In patients with low-grade NMI-BC, 88% of the primary tumors carried a mutation and 88% of the recurrences were mutant.
Conclusions/significance: The mutation assays present a companion diagnostic to define patients for targeted therapies. In addition, the assays are a potential biomarker to detect recurrences during surveillance. We showed that 88% of patients presenting with low-grade NMI-BC are eligible for such a follow-up. This may contribute to a reduction in the number of cystoscopical examinations.
Conflict of interest statement
Figures

References
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Black PC, Agarwal PK, Dinney CP. Targeted therapies in bladder cancer–an update. Urol Oncol. 2007;25:433–438. - PubMed
-
- Gomez-Roman JJ, Saenz P, Molina M, Cuevas Gonzalez J, Escuredo K, et al. Fibroblast growth factor receptor 3 is overexpressed in urinary tract carcinomas and modulates the neoplastic cell growth. Clin Cancer Res. 2005;11:459–465. - PubMed
-
- Martinez-Torrecuadrada JL, Cheung LH, Lopez-Serra P, Barderas R, Canamero M, et al. Antitumor activity of fibroblast growth factor receptor 3-specific immunotoxins in a xenograft mouse model of bladder carcinoma is mediated by apoptosis. Mol Cancer Ther. 2008;7:862–873. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
