

Advances in labor analgesia
- PMID: 21072284
- PMCID: PMC2971706
- DOI: 10.2147/ijwh.s4553
Advances in labor analgesia
Abstract
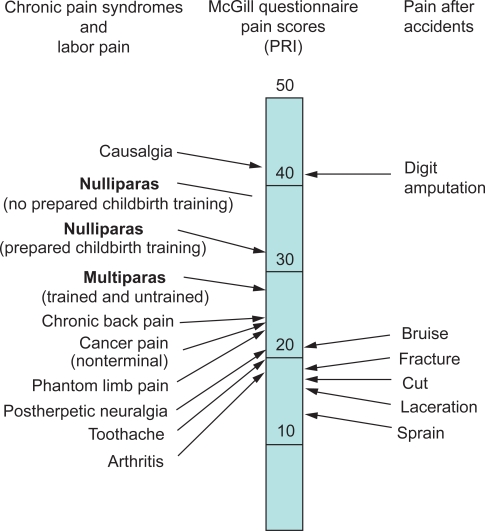
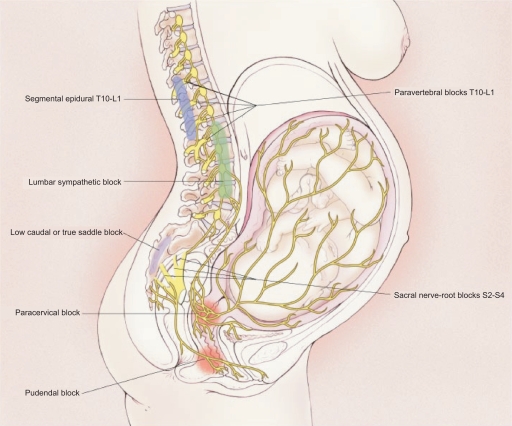
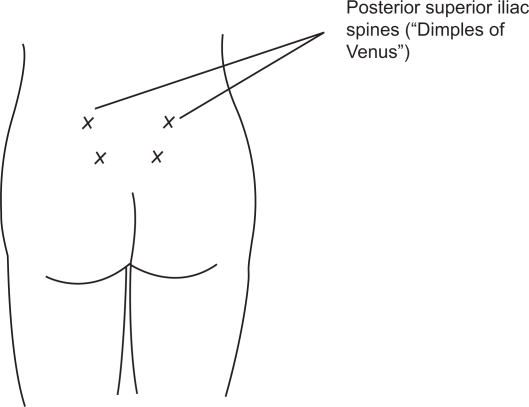
The pain of childbirth is arguably the most severe pain most women will endure in their lifetimes. The pain of the early first stage of labor arises from dilation of the lower uterine segment and cervix. Pain from the late first stage and second stage of labor arises from descent of the fetus in the birth canal, resulting in distension and tearing of tissues in the vagina and perineum. An array of regional nerve blocks, systemic analgesic, and nonpharmacologic techniques are currently used for labor analgesia. Nonpharmacologic methods are commonly used, but the effectiveness of these techniques generally lacks rigorous scientific study. Continuous labor support has been shown to decrease the use of pharmacologic analgesia and shorten labor. Intradermal water injections decrease back labor pain. Neuraxial labor analgesia (most commonly epidural or combined spinal-epidural) is the most effective method of pain relief during childbirth, and the only method that provides complete analgesia without maternal or fetal sedation. Current techniques commonly combine a low dose of local anesthetic (bupivacaine or ropivacaine) with a lipid soluble opioid (fentanyl or sufentanil). Neuraxial analgesia does not increase the rate of cesarean delivery compared to systemic opioid analgesia; however, dense neuraxial analgesia may increase the risk of instrumental vaginal delivery.
Keywords: childbirth pain; epidural analgesia; labor analgesia; neuraxial analgesia.
Figures

References
-
- von Steinbüchel R. Vorläufige Mitteilung über die Anwendung des Skopolamin-Morphium-Injektionen in der Geburtshilfe. Zentrallblatt Gyn. 1902;30:1304–1306.
-
- Caton D. The history of obstetric anesthesia. In: Chestnut DH, Polley LS, Tsen LC, Wong CA, editors. Obstetric Anesthesia Principles and Practice. 4th ed. Philadelphia: Elsevier Mosby; 2009. pp. 3–13.
-
- Hingson RA, Edwards WB. Continuous caudal analgesia: An analysis of the first ten thousand confinements thus managed with the report of the authors’ first thousand cases. JAMA. 1943;123:538–546.
-
- Melzack R. The myth of painless childbirth (the John J. Bonica lecture) Pain. 1984;19(4):321–337. - PubMed
-
- Wong CA. Obstetric Pain. In: Ballantyne JC, Rathmell JP, Fishman SM, editors. Bonica’s Management of Pain. 4th ed. Philadelphia: Lippincott Williams & Wilkins; In press.
LinkOut - more resources
Full Text Sources
Medical
