

WEB downloadable software for training in cardiovascular hemodynamics in the (3-D) stress echo lab
- PMID: 21073738
- PMCID: PMC2997766
- DOI: 10.1186/1476-7120-8-48
WEB downloadable software for training in cardiovascular hemodynamics in the (3-D) stress echo lab
Abstract
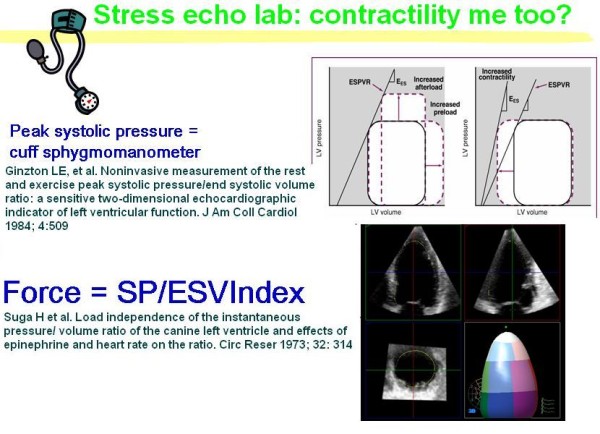
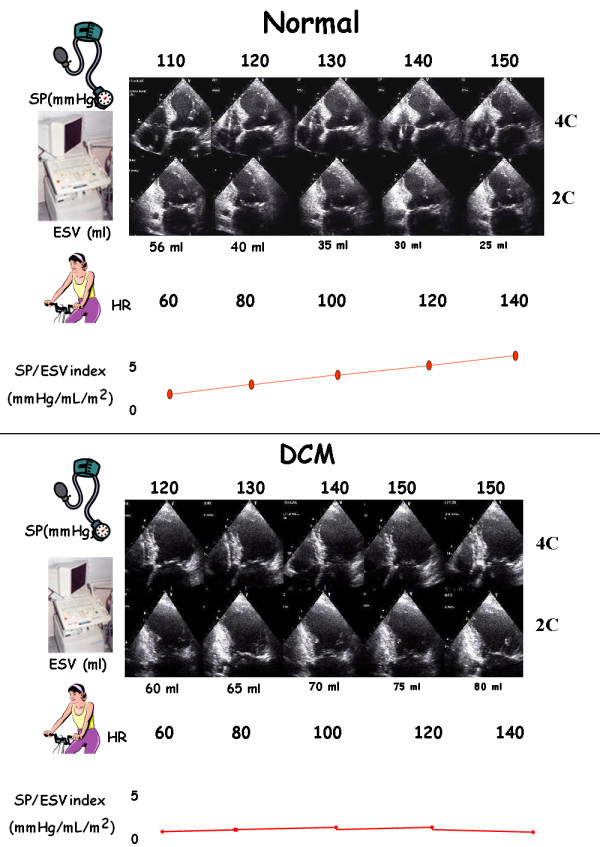
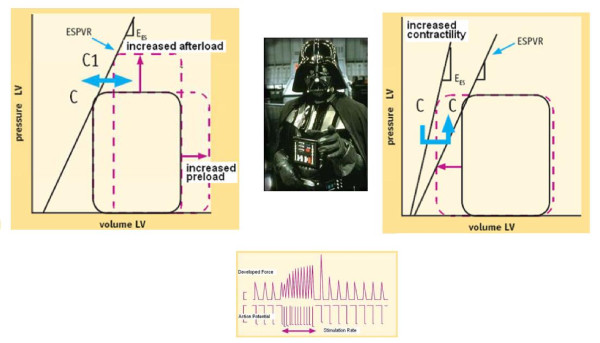
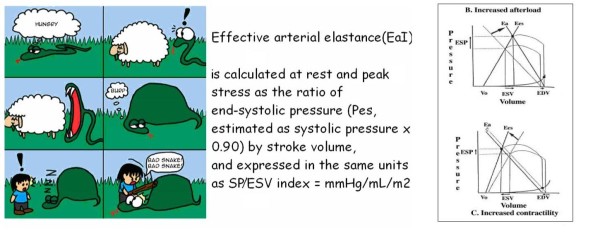
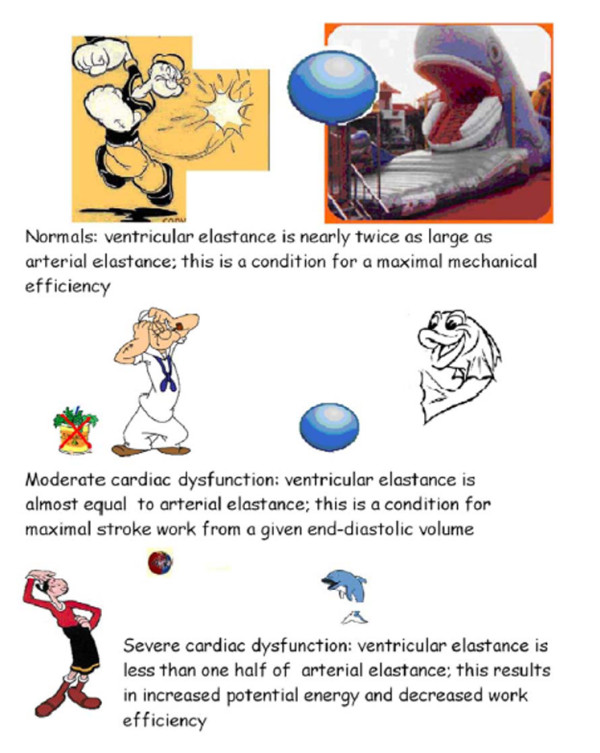
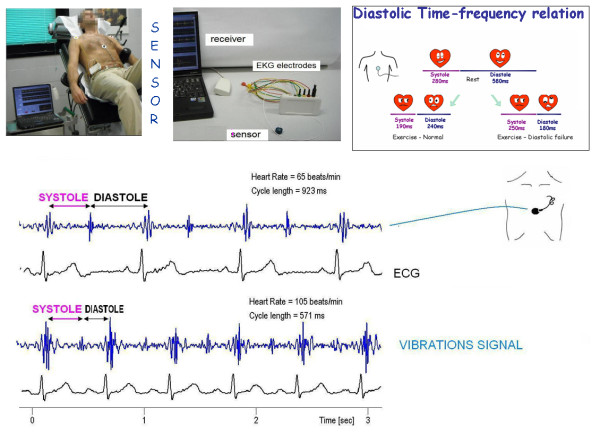
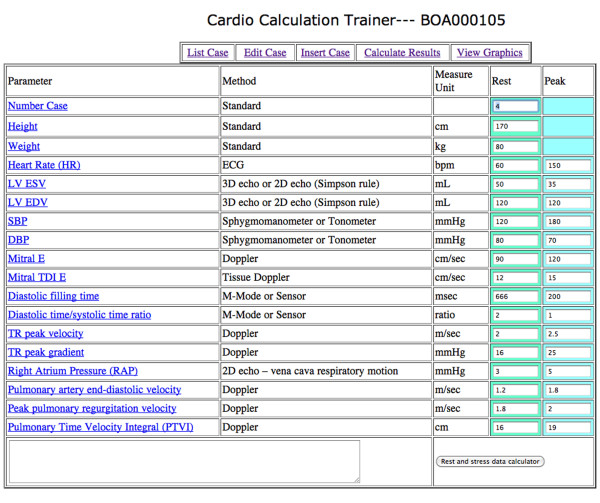
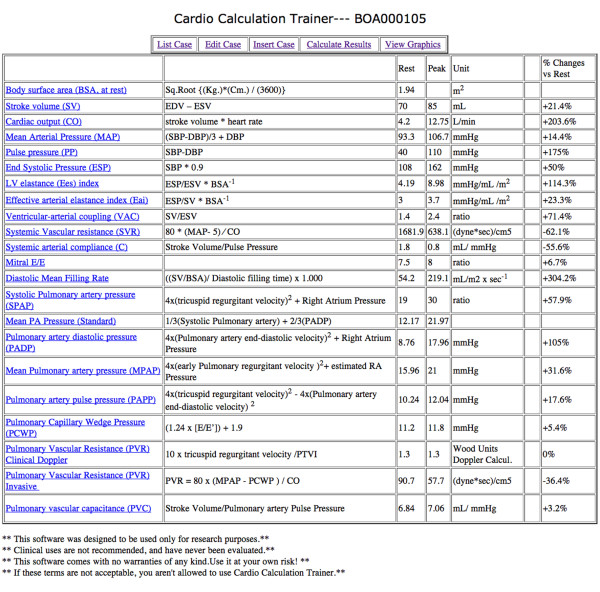
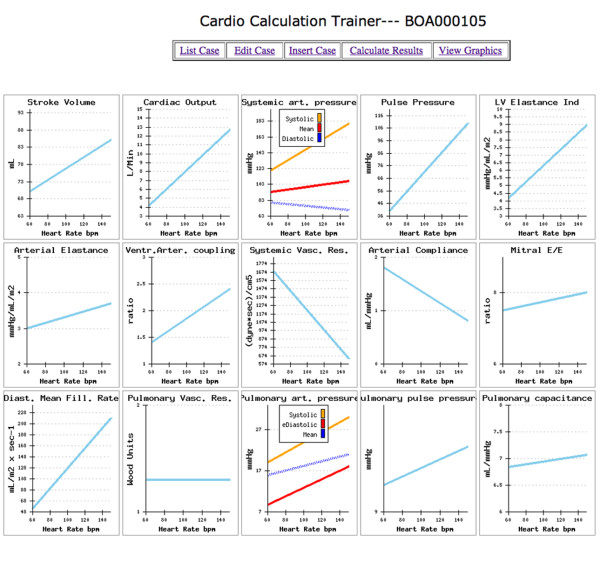
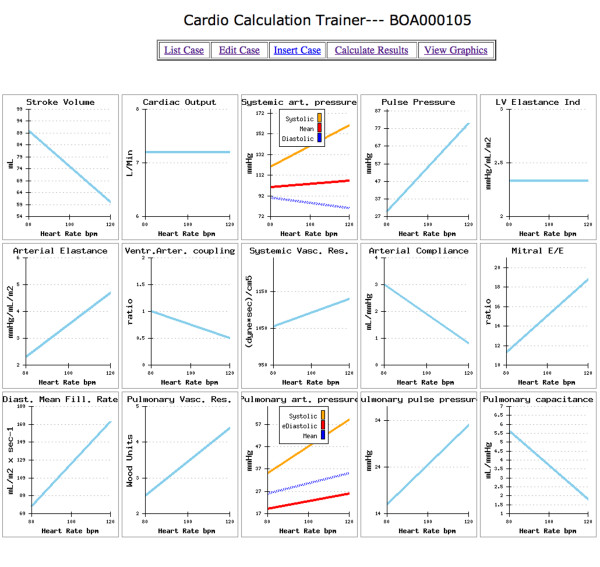
When a physiological (exercise) stress echo is scheduled, interest focuses on wall motion segmental contraction abnormalities to diagnose ischemic response to stress, and on left ventricular ejection fraction to assess contractile reserve. Echocardiographic evaluation of volumes (plus standard assessment of heart rate and blood pressure) is ideally suited for the quantitative and accurate calculation of a set of parameters allowing a complete characterization of cardiovascular hemodynamics (including cardiac output and systemic vascular resistance), left ventricular elastance (mirroring left ventricular contractility, theoretically independent of preload and afterload changes heavily affecting the ejection fraction), arterial elastance, ventricular arterial coupling (a central determinant of net cardiovascular performance in normal and pathological conditions), and diastolic function (through the diastolic mean filling rate). All these parameters were previously inaccessible, inaccurate or labor-intensive and now become, at least in principle, available in the stress echocardiography laboratory since all of them need an accurate estimation of left ventricular volumes and stroke volume, easily derived from 3 D echo. Aims of this paper are: 1) to propose a simple method to assess a set of parameters allowing a complete characterization of cardiovascular hemodynamics in the stress echo lab, from basic measurements to calculations 2) to propose a simple, web-based software program, to learn and training calculations as a phantom of the everyday activity in the busy stress echo lab 3) to show examples of software testing in a way that proves its value.The informatics infrastructure is available on the web, linking to http://cctrainer.ifc.cnr.it.
Figures
References
-
- Picano E. Stress Echocardiography. 5. Springer-Verlag Berlin Heidelberg; 2009.
-
- Jacobs LD, Salgo IS, Goonewardena S, Weinert L, Coon P, Bardo D, Gerard O, Allain P, Zamorano JL, de Isla LP, Mor-Avi V, Lang RM. Rapid online quantification of left ventricular volume from real-time three-dimensional echocardiographic data. Eur Heart J. 2006;27:460–468. doi: 10.1093/eurheartj/ehi666. - DOI - PubMed
-
- Delgado V, Bax JJ, Van Der Wall EE. Towards assessment of left ventricular mechanics in true three dimensions. Eur Heart J. 2009;30:554–55. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
