

Review
doi: 10.1016/j.suc.2010.08.006.
Unusual causes of cutaneous ulceration
Affiliations
- PMID: 21074034
- PMCID: PMC2991050
- DOI: 10.1016/j.suc.2010.08.006
Item in Clipboard
Review
Unusual causes of cutaneous ulceration
Surg Clin North Am.
2010 Dec.
Abstract
Skin ulceration is a major source of morbidity and is often difficult to manage. Ulcers caused by an inflammatory cause or microvascular occlusion are particularly challenging in terms of diagnosis and treatment. The management of such ulcers requires careful assessment of associated systemic conditions and a thorough analysis of the ulcer's clinical and histologic findings. In this article, the authors discuss several examples of inflammatory ulcers and the approach to the diagnosis and treatment of these ulcers.
Copyright © 2010 Elsevier Inc. All rights reserved.
Figures
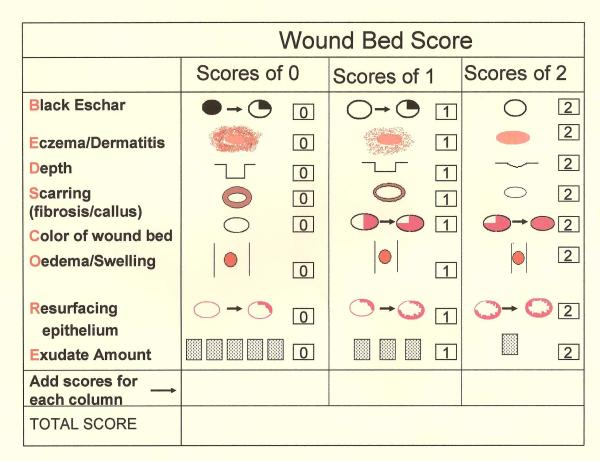
The total WBS adds each individual score for each characteristic to give a total score.  Percent of eschar present(>25, 1–25%, none);
Percent of eschar present(>25, 1–25%, none);  Severity of peri-ulcer dermatitis (severe, moderate, none or mild);
Severity of peri-ulcer dermatitis (severe, moderate, none or mild);  Depth of the wound (severely depressed or raised compared to peri-wound skin);
Depth of the wound (severely depressed or raised compared to peri-wound skin);  Severity of callus/fibrosis (severe, moderate, none or minimal);
Severity of callus/fibrosis (severe, moderate, none or minimal);  Percent of pink granulation tissue present (<50%, 50–75%, >75%);
Percent of pink granulation tissue present (<50%, 50–75%, >75%);  Severity of edema (severe, moderate, none/mild);
Severity of edema (severe, moderate, none/mild);  Percent of healing edges (<25%, 25–75%, >75%);
Percent of healing edges (<25%, 25–75%, >75%);  Frequency of dressing changes (severe, moderate, none/mild)
Frequency of dressing changes (severe, moderate, none/mild)
Percent of eschar present(>25, 1–25%, none); Severity of peri-ulcer dermatitis (severe, moderate, none or mild); Depth of the wound (severely depressed or raised compared to peri-wound skin); Severity of callus/fibrosis (severe, moderate, none or minimal); Percent of pink granulation tissue present (<50%, 50–75%, >75%); Severity of edema (severe, moderate, none/mild); Percent of healing edges (<25%, 25–75%, >75%); Frequency of dressing changes (severe, moderate, none/mild)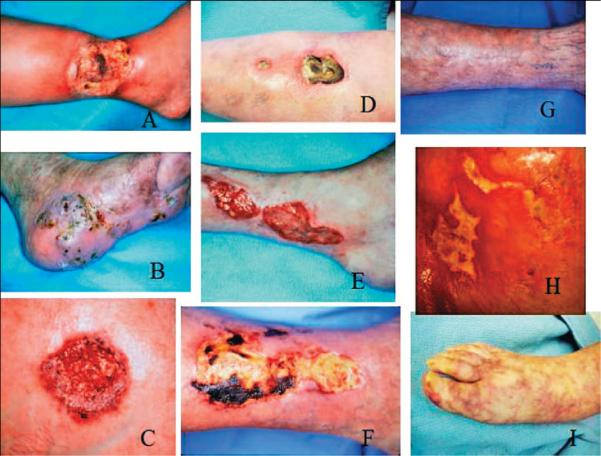
(A) Pyoderma gangrenosum in a patient with rheumatoid arthritis. (B) The more `granulomatous' appearance of Pyoderma gangrenosum. (C) Typical Pyoderma gangrenosum with purple edges. (D) Undermined ulcer of Pyoderma gangrenosum. (E) The undulating borders of a rheumatoid ulcer. (F) Eschar in an ulcer due to polyarteritis nodosa. (G) Same patient shown in (F), after successful use of immunosuppressants. (H) The `angular' ulcers seen in patients with collagen vascular diseases, often mimicking factitial ulcers. (I) Livedo reticularis and small ulcers in a patient with cholesterol embolization.

(A) The appearance of a PG ulcer prior to treatment. (B) Dramatic impovement after second day of pulse methylprednisolone. (C) Six days after pulse steroids the ulcers decreased markedly in size. (D) Healed ulcer 3 weeks after treatment.
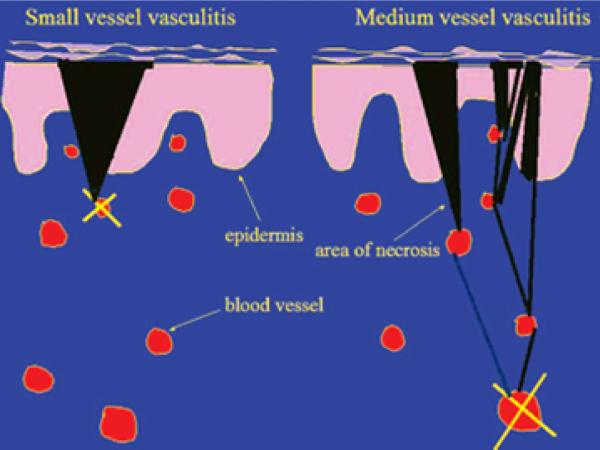
A superficial vasculitis (left side of diagram) leads to a wedge-shaped area of necrosis and, thus, a well defined and regular skin purpura or necrosis. Conversely, occlusion of a deep vessel (right side of diagram) leaves open the chance for anastomosing vessels to alter the effect at the skin.

Excisional biopsy marked on edge of ulcer including surrounding erythema.
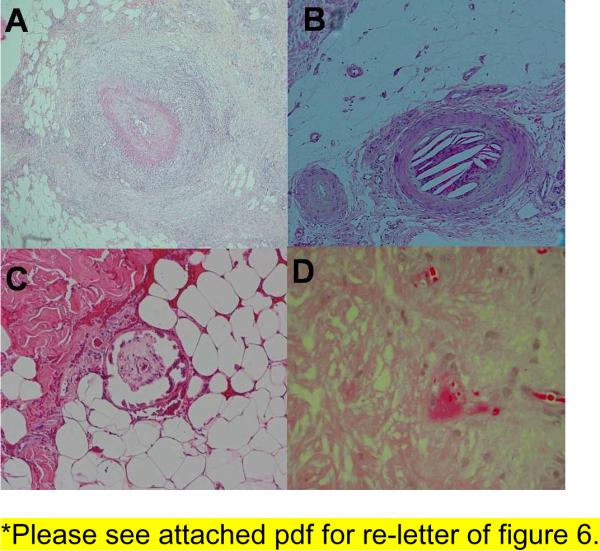
(A) Dense inflammation around a medium sized artery seen in polyarteritis nodosa. (B) Cleft like spaces inside a vessel seen in cholesterol emboli. (C) Fibrin thrombi inside a vessel seen in cryofibrinogenemia. (D) Calcification of medial layer of a blood vessel seen in calciphylaxis.

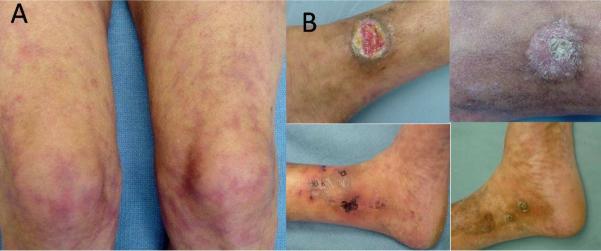
(A) Painful ulcer with background livedo reticularis. (B) Worsening ulcer not responsive to pulse steroids, azathioprine, pentoxifylline, antibiotics and debridement. Skin biopsy showed calciphylaxis. (C) Repeat debridement, IV antibiotics, bioengineered skin applied to ulcer with good response; Azathioprine discontinued after one month, compression therapy, pain management, antiseptic dressings were used.(D) Ulcer healed after 3 months.
(A) Typical presentation of livedo reticularis. (B) Ulcers healed with compression pentoxifylline and colchicine.
References
-
- Panuncialman J, Falanga V. The science of wound bed preparation. Clin Plast Surg. 2007 Oct;34(4):621–632. - PubMed
-
- Brunsting LA, Goeckerman WH, O'Leary PA. Pyoderma (echthyma) gangrenosum: clinical and experimental observations in 5 cases occuring in adults. Arch Dermatol Syphilol. 1930;22:655–680.
-
- Weenig RH, Davis MD, Dahl PR, Su WP. Skin ulcers misdiagnosed as pyoderma gangrenosum. N Engl J Med. 2002 Oct 31;347(18):1412–1418. - PubMed
-
- Powell FC, Schroeter AL, Su WP, Perry HO. Pyoderma gangrenosum: a review of 86 patients. Q J Med. 1985 May;55(217):173–186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
