

Management for prostate cancer treatment related posterior urethral and bladder neck stenosis with stents
- PMID: 21074796
- PMCID: PMC3557853
- DOI: 10.1016/j.juro.2010.09.020
Management for prostate cancer treatment related posterior urethral and bladder neck stenosis with stents
Abstract
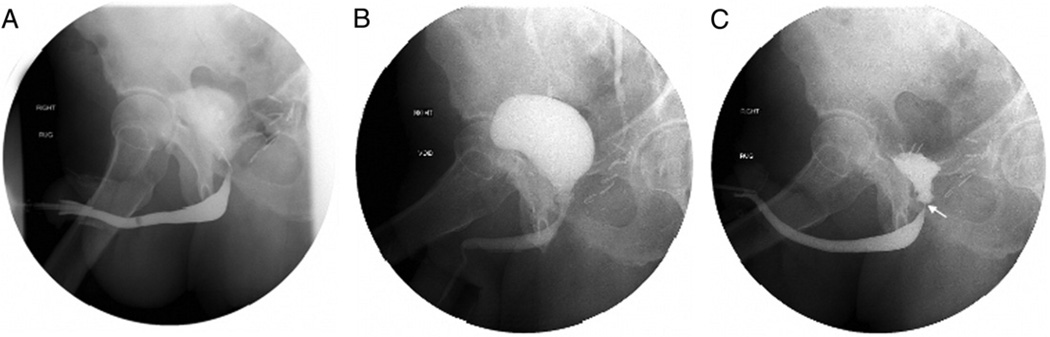
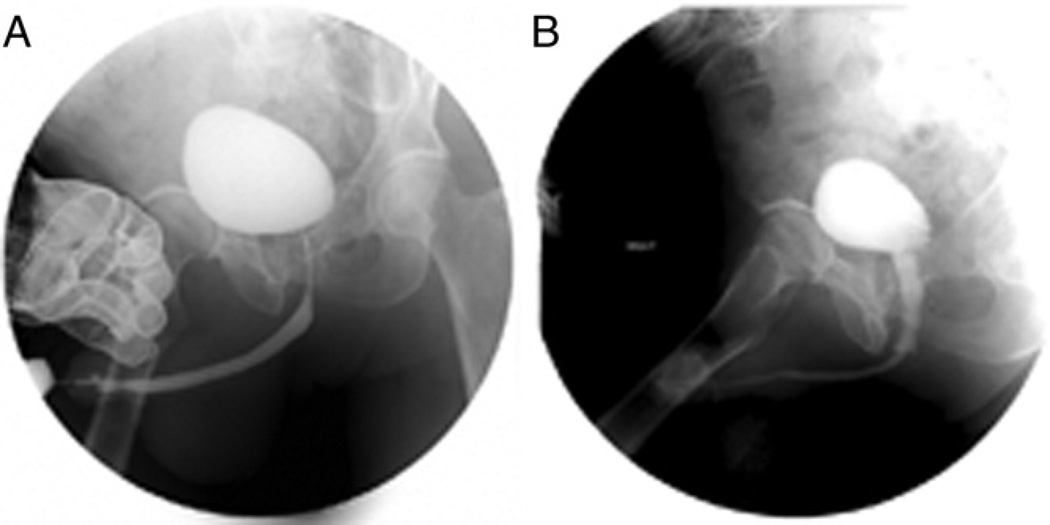
Purpose: Prostate cancer treatment has the potential to lead to posterior urethral stricture. These strictures are sometimes recalcitrant to dilation and urethrotomy alone. We present our experience with the Urolume® stent for prostate cancer treatment related stricture.
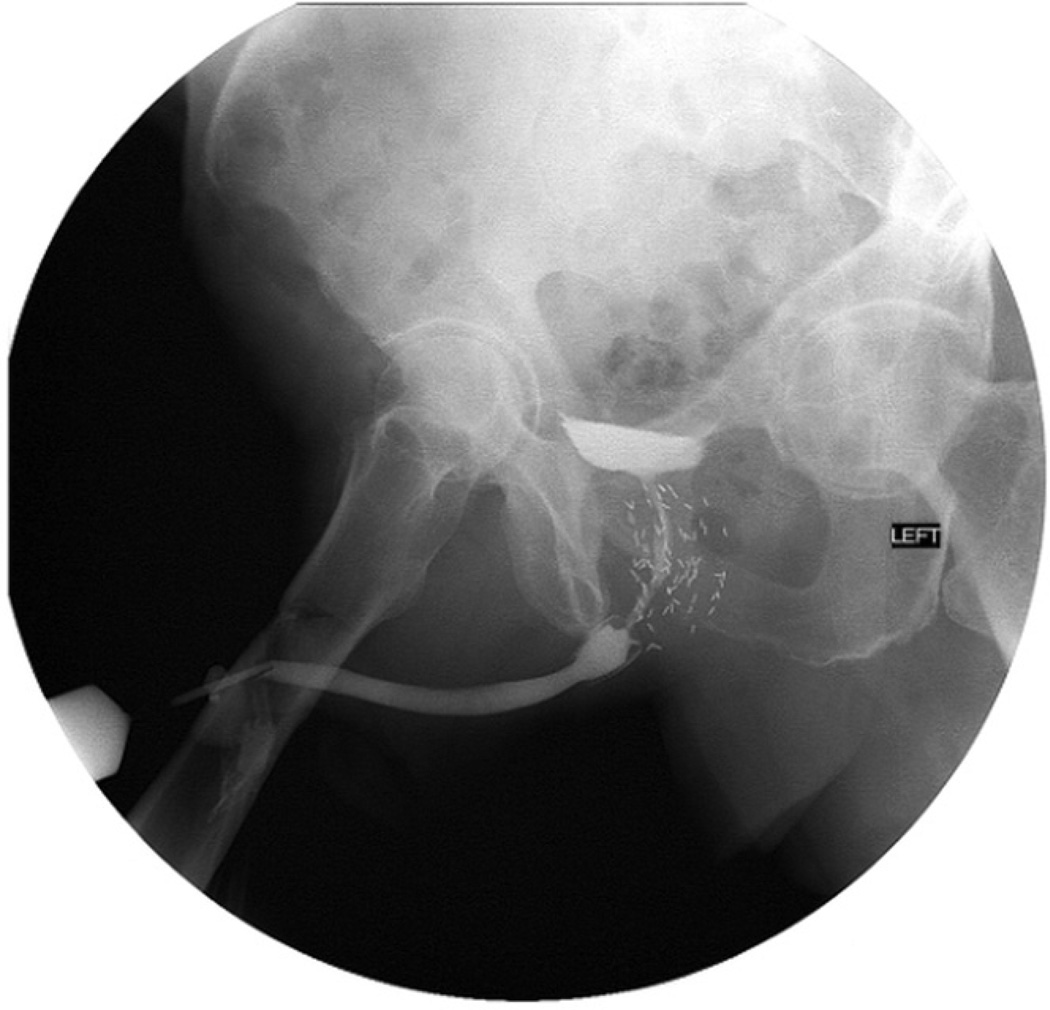
Materials and methods: A total of 38 men with posterior urethral stricture secondary to prostate cancer treatment were treated with Urolume stenting. Stents were placed in all men after aggressive urethrotomy over the entire stricture. A successfully managed stricture was defined as open and stable for greater than 6 months after any necessary secondary procedures.
Results: The initial success rate was 47%. After a total of 31 secondary procedures in 19 men, including additional stent placement in 8 (18%), the final success rate was 89% at a mean ± SD followup of 2.3 ± 2.5 years. Four cases (11%) in which treatment failed ultimately requiring urinary diversion (3) or salvage prostatectomy (1). Incontinence was noted in 30 men (82%), of whom 19 (63%) received an artificial urinary sphincter a mean of 7.2 ± 2.4 months after the stent. Subanalysis revealed that irradiated men had longer strictures (3.6 vs 2.0 cm, p = 0.003) and a higher post-stent incontinence rate (96% vs 50%, p < 0.001) than men who underwent prostatectomy alone but the initial failure rate was similar (54% vs 50%, p = 0.4).
Conclusions: Urolume stenting is a reasonable option for severe post-prostate cancer treatment stricture when patients are unwilling or unable to undergo open reconstructive surgery. Incontinence should be expected. The need for additional procedures is common and in some men may be required periodically for the lifetime of the stent.
Copyright © 2011 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- American Cancer Society. [Accessed February 10, 2009]; Available at http://www.cancer.org.
-
- Elliott SP, Meng MV, Elkin EP, et al. Incidence of urethral stricture after primary treatment for prostate cancer: data from CaPSURE. J Urol. 2007;178:529. - PubMed
-
- Merrick GS, Butler WM, Wallner KE, et al. Risk factors for the development of prostate brachytherapy related urethral strictures. J Urol. 2006;175:1376. - PubMed
-
- Allen ZA, Merrick GS, Butler WM, et al. Detailed urethral dosimetry in the evaluation of prostate brachytherapy-related urinary morbidity. Int J Radiat Oncol Biol Phys. 2005;62:981. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
