

Targeting atrioventricular differences in ion channel properties for terminating acute atrial fibrillation in pigs
- PMID: 21076156
- PMCID: PMC3306132
- DOI: 10.1093/cvr/cvq359
Targeting atrioventricular differences in ion channel properties for terminating acute atrial fibrillation in pigs
Erratum in
- Cardiovasc Res. 2011 Nov 1;92(2):358
Abstract
Aims: The goal was to terminate atrial fibrillation (AF) by targeting atrioventricular differences in ionic properties.
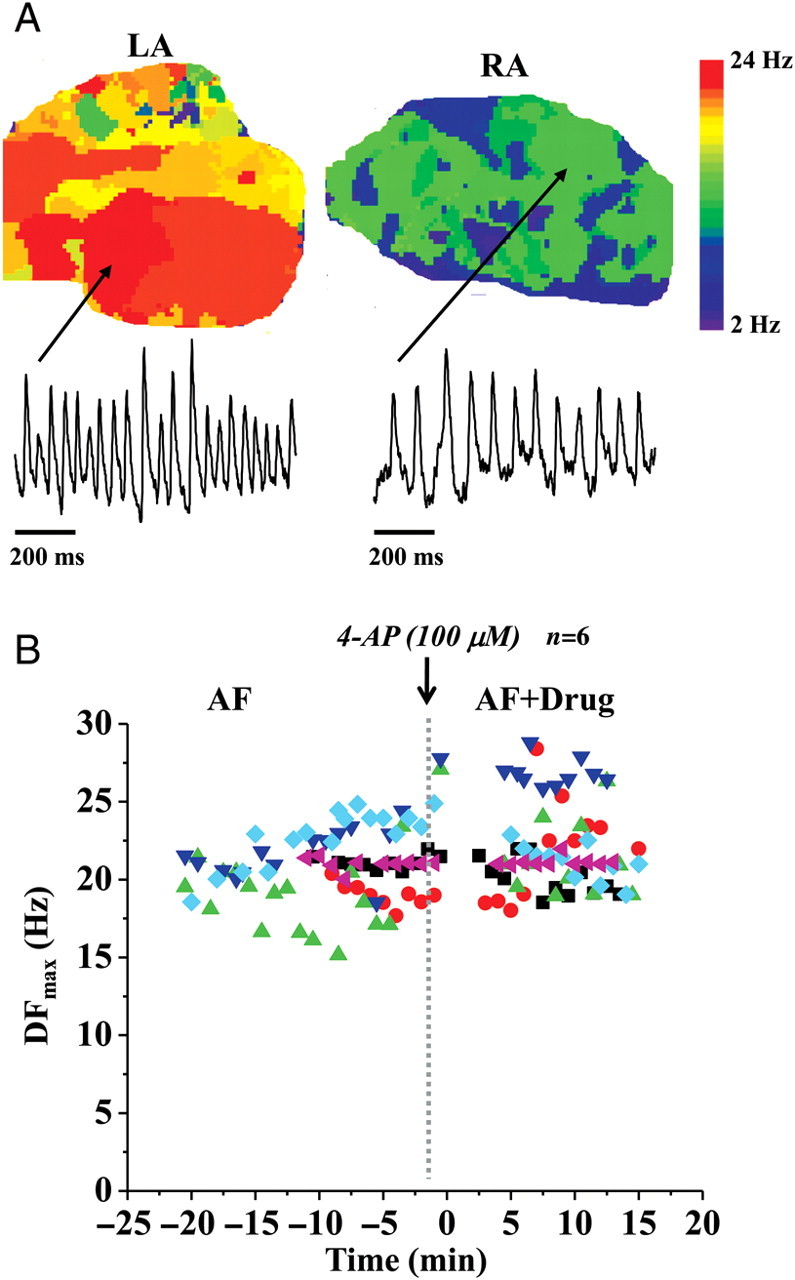
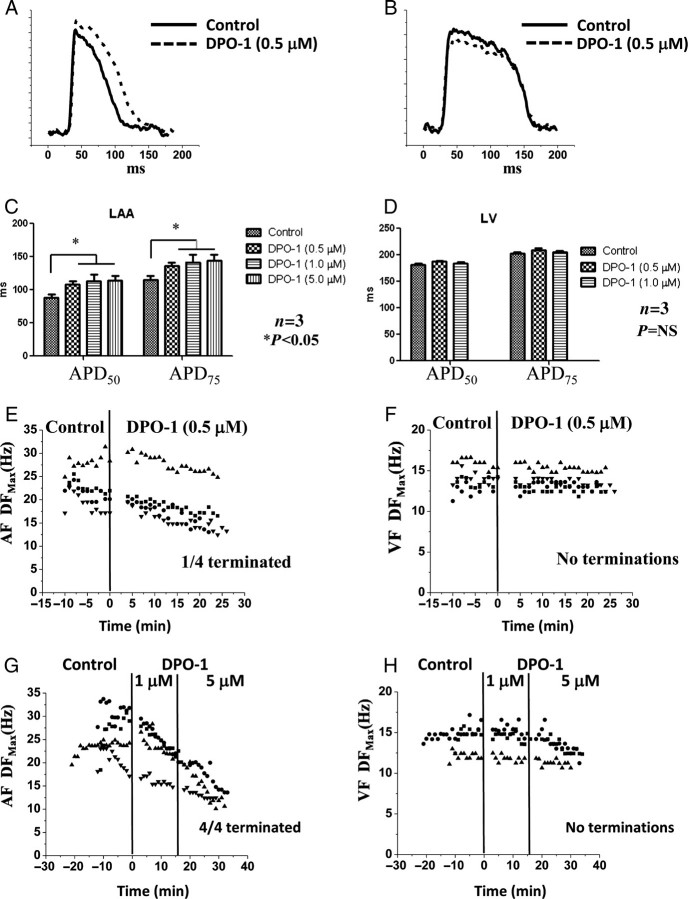
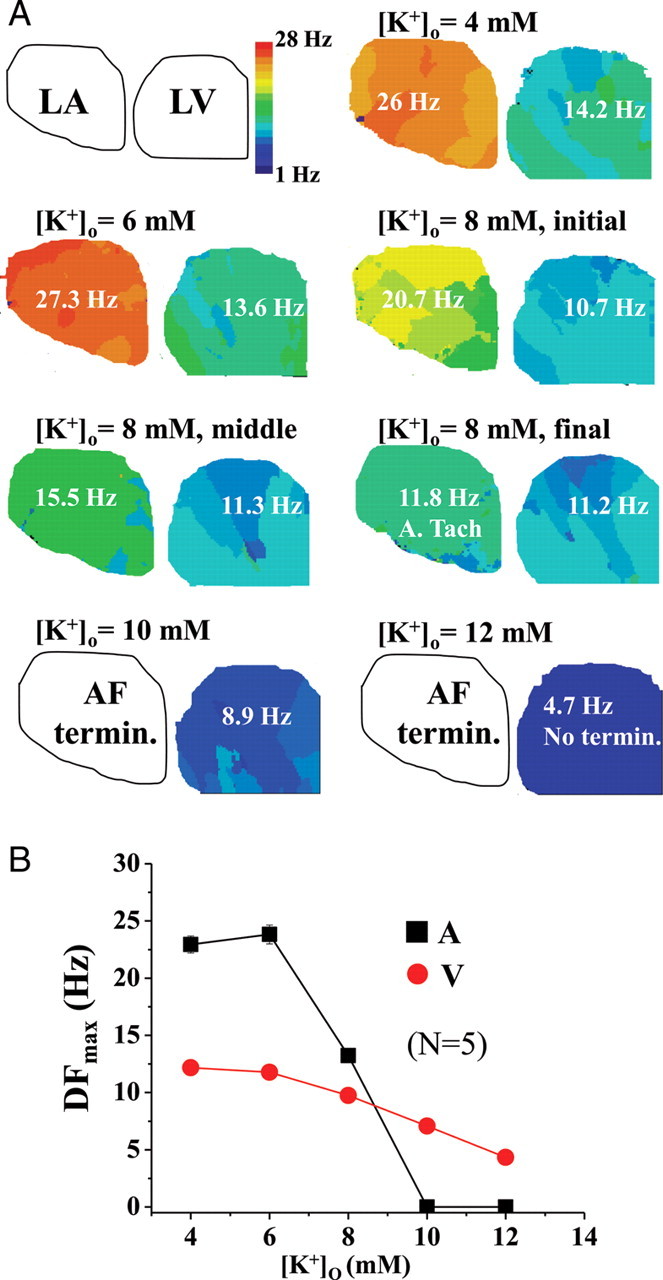
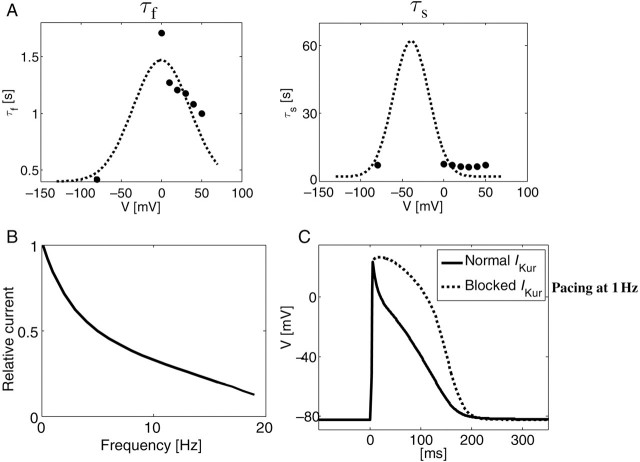
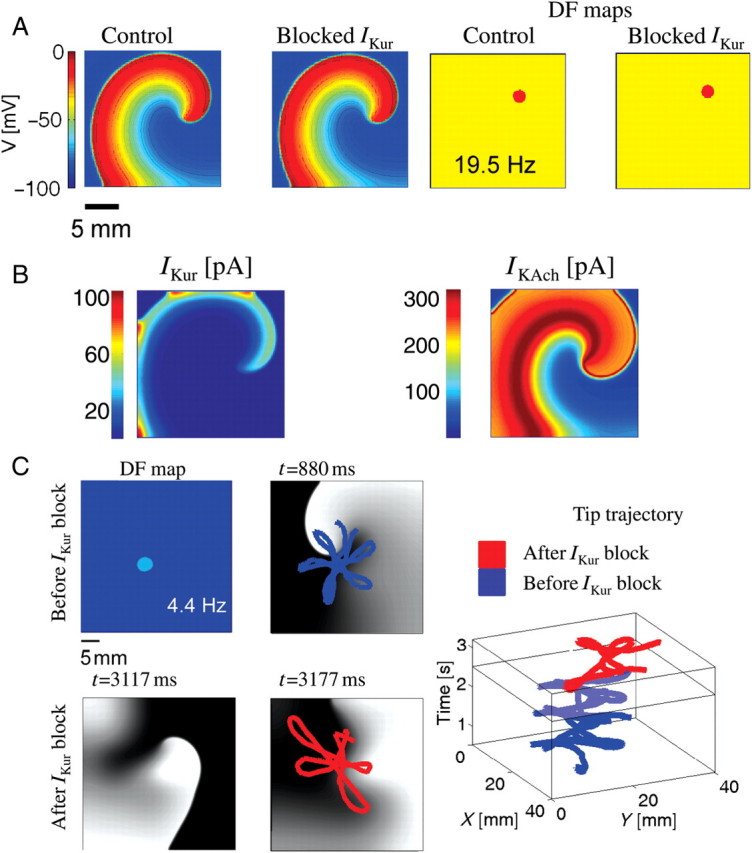
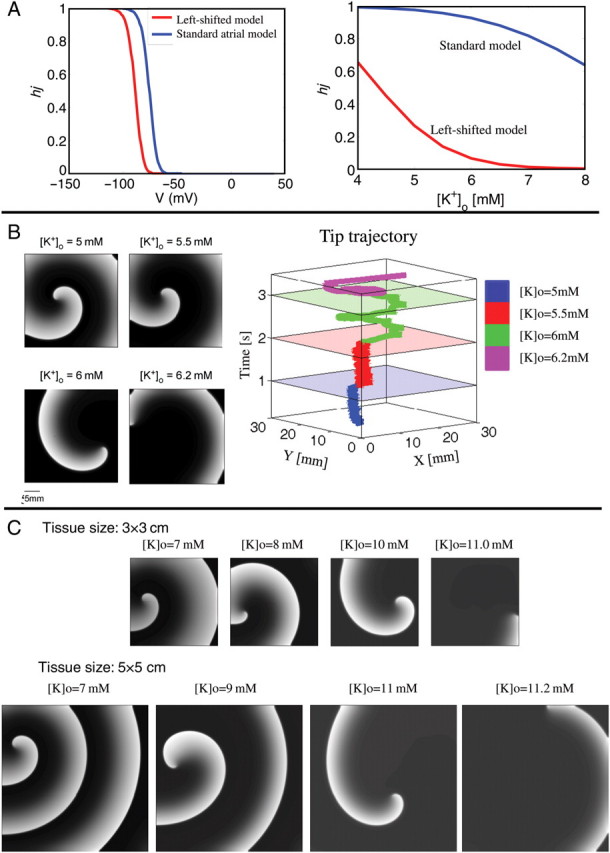
Methods and results: Optical mapping was used to record electrical activity during carbachol (0.25-0.5 μM)-induced AF in pig hearts. The atrial-specific current, I(Kur), was blocked with 100 μM 4-aminopyridine (4-AP) or with 0.5 μM DPO-1. Hearts in AF and ventricular fibrillation (VF) were also subjected to increasing levels of extracellular K(+) ([K(+)](o): 6-12 mM), compared with controls (4 mM). We hypothesized that due to the more negative steady-state half inactivation voltage for the atrial Na(+) current, I(Na), compared with the ventricle, AF would terminate before VF in hyperkalaemia. Mathematical models were used to interpret experimental findings. The I(Kur) block did not terminate AF in a majority of experiments (6/9 with 4-AP and 3/4 with DPO-1). AF terminated in mild hyperkalaemia ([K(+)](o) ≤ 10.0 mM; N = 8). In contrast, only two of five VF episodes terminated at the maximum ([K(+)](o): 12 mM [K(+)](o)). The I(Kur) block did not terminate a simulated rotor in cholinergic AF because its contribution to repolarization was dwarfed by the large magnitude of the acetylcholine-activated K(+) current (I(K,ACh)). Simulations showed that the lower availability of the atrial Na(+) current at depolarized potentials, and a smaller atrial tissue size compared with the ventricle, could partly explain the earlier termination of AF compared with VF during hyperkalaemia.
Conclusion: I(Kur) is an ineffective anti-arrhythmic drug target in cholinergic AF. Manipulating Na(+) current 'availability' might represent a viable anti-arrhythmic strategy in AF.
Figures
References
-
- Nattel S. New ideas about atrial fibrillation 50 years on. Nature. 2002;415:219–226. doi:10.1038/415219a. - DOI - PubMed
-
- Page RL, Roden DM. Drug therapy for atrial fibrillation: where do we go from here? Nat Rev Drug Discov. 2005;4:899–910. doi:10.1038/nrd1876. - DOI - PubMed
-
- Ehrlich JR, Nattel S. Atrial-selective pharmacological therapy for atrial fibrillation: hype or hope? Curr Opin Cardiol. 2009;24:50–55. doi:10.1097/HCO.0b013e32831bc336. - DOI - PubMed
-
- Gaborit N, Le Bouter S, Szuts V, Varro A, Escande D, Nattel S, et al. Regional and tissue specific transcript signatures of ion channel genes in the non-diseased human heart. J Physiol. 2007;582:675–693. doi:10.1113/jphysiol.2006.126714. - DOI - PMC - PubMed
-
- Blaauw Y, Gögelein H, Tieleman RG, van Hunnik A, Schotten U, Allessie MA. Early' class III drugs for the treatment of atrial fibrillation: efficacy and atrial selectivity of AVE0118 in remodeled atria of the goat. Circulation. 2004;110:1717–1724. doi:10.1161/01.CIR.0000143050.22291.2E. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
