

Progression and regression of premalignant cervical lesions in HIV-infected women from Soweto: a prospective cohort
- PMID: 21076276
- PMCID: PMC3166782
- DOI: 10.1097/QAD.0b013e328340fd99
Progression and regression of premalignant cervical lesions in HIV-infected women from Soweto: a prospective cohort
Abstract
Objective: To ascertain progression and regression of cervical dysplasia in HIV-infected women in Soweto.
Design: Prospective cohort.
Methods: Women attending an HIV wellness clinic were offered cervical smears as part of care; smears were assessed using the Bethesda system. Those with high-grade lesions or worse were referred for colposcopy. Progression analyses included women with at least two smears at least 5.5 months apart. Hazard ratios were used to ascertain predictors of progression.
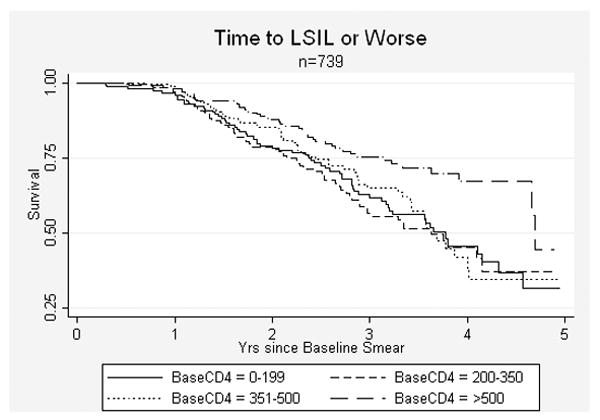
Results: Two thousand, three hundred and twenty-five women had a baseline smear; their median age and CD4 cell count was 32 years and 312 cells/μl, respectively; 17% were taking highly active antiretroviral therapy (HAART); 62, 20 and 14% had normal, low-grade squamous intraepithelial lesions (LSIL) or high-grade squamous intraepithelial lesions (HSIL), respectively. Of those with baseline normal or LSIL smears, 1074 had another smear; progression from normal to LSIL was 9.6/100 person-years (95% CI 8.3-11.1) and progression from normal or LSIL to HSIL was 4.6/100 person-years (95% CI 3.9-5.5). Of 225 women with LSIL at baseline and at least one subsequent smear at least 11.5 months later, 44.0% regressed to normal (21.2/100 person-years (95% CI 17.5-25.7)). Multivariate models suggested increasing risk for progression in women with CD4 cell count below 500 cells/μl and HAART may reduce the risk of progression [adjusted hazard ratio (aHR) 0.72 (0.52-0.99)].
Conclusion: HIV-infected women have high rates of prevalent and incident HSIL and LSIL with relatively low risk of regression to normal from LSIL. HAART appears to protect against progression. Our findings suggest cervical screening intervals should be less than 10 years - irrespective of age in women with CD4 cell counts below 500 cells/μl.
Conflict of interest statement
None of the authors report a conflict of interest.
Figures
Similar articles
-
Increased regression and decreased incidence of human papillomavirus-related cervical lesions among HIV-infected women on HAART.AIDS. 2012 Aug 24;26(13):1645-52. doi: 10.1097/QAD.0b013e32835536a3. AIDS. 2012. PMID: 22555167 Free PMC article.
-
Evolution of cervical abnormalities among women with HIV-1: evidence from surveillance cytology in the women's interagency HIV study.J Acquir Immune Defic Syndr. 2001 Aug 15;27(5):432-42. doi: 10.1097/00126334-200108150-00003. J Acquir Immune Defic Syndr. 2001. PMID: 11511819
-
Incidence of cervical squamous intraepithelial lesions associated with HIV serostatus, CD4 cell counts, and human papillomavirus test results.JAMA. 2005 Mar 23;293(12):1471-6. doi: 10.1001/jama.293.12.1471. JAMA. 2005. PMID: 15784870
-
Clinical importance of "low-grade squamous intraepithelial lesion, cannot exclude high-grade squamous intraepithelial lesion (LSIL-H)" terminology for cervical smears 5-year analysis of the positive predictive value of LSIL-H compared with ASC-H, LSIL, and HSIL in the detection of high-grade cervical lesions with a review of the literature.Gynecol Oncol. 2011 Apr;121(1):152-6. doi: 10.1016/j.ygyno.2010.12.004. Epub 2011 Jan 5. Gynecol Oncol. 2011. PMID: 21211831 Review.
-
HIV-positive women have higher risk of human papilloma virus infection, precancerous lesions, and cervical cancer.AIDS. 2018 Mar 27;32(6):795-808. doi: 10.1097/QAD.0000000000001765. AIDS. 2018. PMID: 29369827 Free PMC article.
Cited by
-
Comparing Papanicolau smear, visual inspection with acetic acid and human papillomavirus cervical cancer screening methods among HIV-positive women by immune status and antiretroviral therapy.AIDS. 2013 Nov 28;27(18):2909-19. doi: 10.1097/01.aids.0000432472.92120.1b. AIDS. 2013. PMID: 23842133 Free PMC article.
-
Cervical cancer awareness and presence of abnormal cytology among HIV-infected women on antiretroviral therapy in rural Andhra Pradesh, India.Int J STD AIDS. 2019 May;30(6):586-595. doi: 10.1177/0956462419825950. Epub 2019 Feb 27. Int J STD AIDS. 2019. PMID: 30813859 Free PMC article.
-
A qualitative analysis of factors influencing HPV vaccine uptake in Soweto, South Africa among adolescents and their caregivers.PLoS One. 2013 Aug 30;8(8):e72094. doi: 10.1371/journal.pone.0072094. eCollection 2013. PLoS One. 2013. PMID: 24023613 Free PMC article.
-
Cost-effectiveness analysis of human papillomavirus vaccination in South Africa accounting for human immunodeficiency virus prevalence.BMC Infect Dis. 2015 Dec 11;15:566. doi: 10.1186/s12879-015-1295-z. BMC Infect Dis. 2015. PMID: 26652918 Free PMC article.
-
Cervical cancer prevention and treatment research in Africa: a systematic review from a public health perspective.BMC Womens Health. 2016 Jun 4;16:29. doi: 10.1186/s12905-016-0306-6. BMC Womens Health. 2016. PMID: 27259656 Free PMC article.
References
-
- Ferlay J, Bray F, Pisani P, Parkin DM. IARC CancerBase No. 5 version 2.0. Lyon: IARC Press; 2004. GLOBOCAN 2002: Cancer Incidence, Mortality and Prevalence Worldwide.
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- Munoz N, Bosch FX, de Sanjose S, Tafur L, Izarzugaza I, et al. The causal link between human papillomavirus and invasive cervical cancer: a population-based case-control study in Colombia and Spain. Int J Cancer. 1992;52:743–749. - PubMed
-
- Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189:12–19. - PubMed
