

Review
doi: 10.1097/QAD.0b013e328340fd42.
Editorial neuroAIDS review
- PMID: 21076277
- PMCID: PMC4464840
- DOI: 10.1097/QAD.0b013e328340fd42
Item in Clipboard
Review
Editorial neuroAIDS review
AIDS.
.
No abstract available
Figures
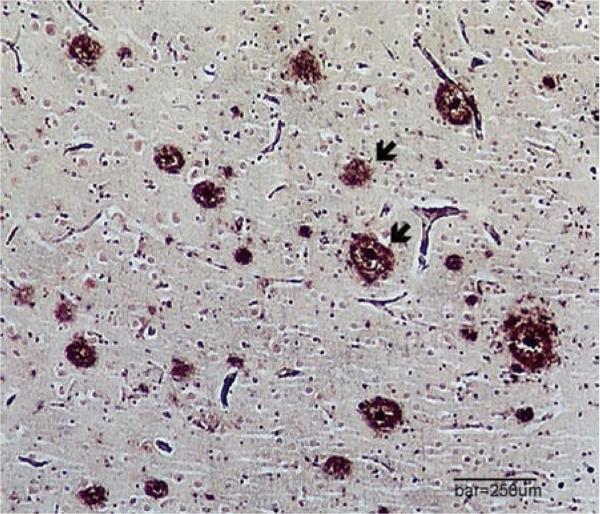
Clinically, HIV-associated neurocognitive disorder was only one factor contributing to her dementia. At death, her brain contained numerous amyloid plaques and tau-neurofibrillary tangles (not shown), typical of AD (modified Bielschowsky silver stain, bar equals 250 μm). AD, Alzheimer's disease.
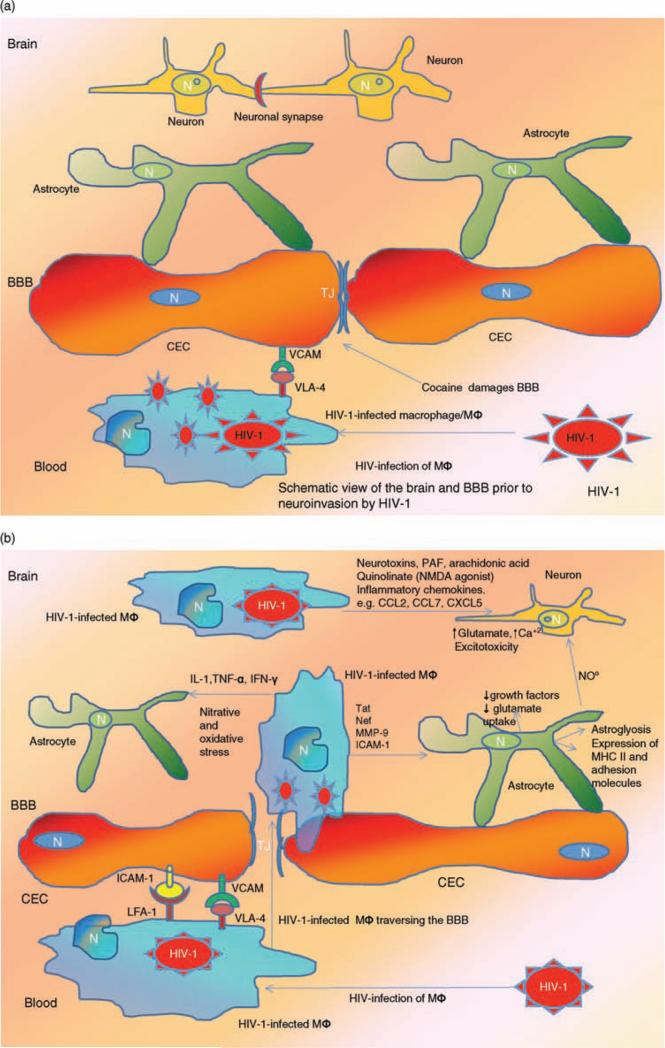
(a) Blood–brain barrier (BBB) prior to infection. Normally, the human BBB, which is composed of interacting adjacent cerebral endothelial cells (CECs) and astrocytes, effectively separates the CNS from cellular and molecular components of the peripheral circulation and creates a unique reservoir environment for functioning neurons and astrocytes among other cells in the brain. Adjacent CECs contain tight junctions (TJs) that serve as the anatomic and functional barrier against harmful molecules from the blood stream. The process of transendothelial migration of HIV-1-infected monocytes involves interactions among adhesion molecules on CECs [e.g. vascular endothelial adhesion molecule (VCAM)] and their ligands on the activated leukocyte [very late antigen-4 (VLA-4)]. During the course of NeuroAIDS, HIV-1-infected macrophage/monocytes from the blood, traverse the TJs of the CECs and infiltrate the brain parenchyma. Once within this milieu, they differentiate into macrophage/microglia (MΦ). Drugs including cocaine and methamphetamine damage the BBB and further facilitate ingress of the HIV-1-infected monocytes into the brain. (b) BBB postinfection. Once within the brain parenchyma, HIV-1-infected MΦ secrete elevated levels of pro-inflammatory cytokines including interleukin-β (IL-β), interferon-γ (IFN-γ), and tumor necrosis factor-α (TNF-α), which in turn activate uninfected macrophage/microglia and adversely affect astrocytes. These pro-inflammatory cytokines also increase BBB permeability and induce further expression of adhesion molecules including VCAM and inter-cellular adhesion molecule (ICAM) by activated CECs, which in turn promote further ingress of HIV-1-infected monocytes into the CNS. In addition to cytokines, inflammatory chemokines contribute to brain inflammation [e.g. chemokine ligand 2 (CCL2); chemokine ligand 7 (CCL7); C-X-C motif chemokine 5 (CXCL5)]. Within the CNS, MFs produce nitric oxide (NO) and promote oxidative injury that affects both astrocytes and CECs. HIV-1-infected MΦs also release HIV-1 Tat protein that induces expression of the adhesion molecules by CECs. Neuronal injury in the context of NeuroAIDS is also promoted by processes including the activation of the N-methyl-D-aspartate receptor (NMDAR)-coupled ion channels, which in turn leads to massive influx of Ca+2 ions. This process then leads to activation of several enzymes including matrix metallo-proteinases, generation of free radicals, and release of glutamate, which cause neuronal apoptosis. Other inflammatory mediators such as platelet activating factor (PAF), arachidonate, and quinolinate (an NMDA agonist) also participate in neuronal injury. HIV-1 infection of astrocytes also leads to astroglyosis and inflammatory cascades. Reproduced with permission from [,,–189].
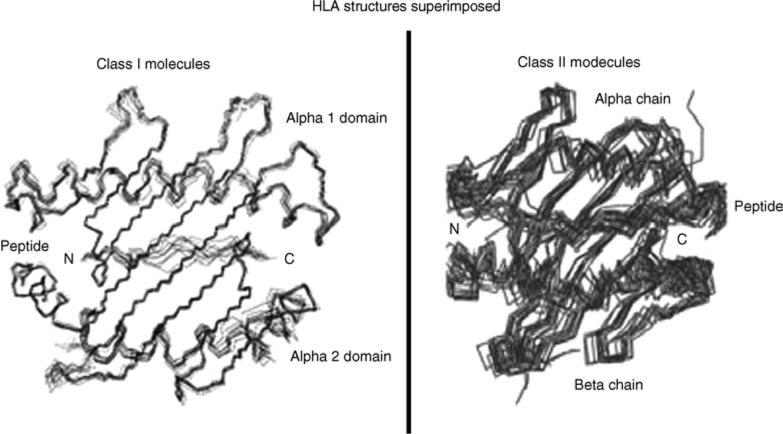
The illustration shows structural features of superimposed multiple short peptides binding to HLA molecules, which is a prerequisite to stimulate T-cell immunity. HLA molecules are often polymorphic across ethnic groups and hence peptide binding specificity varies for each population. Reproduced with permission from [199].
References
-
- Minagar A, Shapshak P. HIV associated dementia: clinical features and pathogenesis. In: Minagar A, Shapshak P, editors. NEURO-AIDS. Nova Science Publ; Hauppauge, New York: 2006.
-
- Fernandez F, Ruiz P, editors. Psychiatric aspects of HIV/AIDS. Lippincott Williams and Wilkins; Philadelphia, PA: 2006.
-
- Goodkin K. Virology, Immunology, Transmission, and disease stage. In: Fernandez F, Ruiz P, editors. Psychiatric aspects of HIV/AIDS. Lippincott Williams and Wilkins; Philadelphia, PA: 2006. pp. 11–22.
-
- Goodkin K, Verma A, Shapshak P, editors. The spectrum of NeuroAIDS disorders: pathophysiology, diagnosis, and treatment. ASM Press; Washington, DC: 2008.
Publication types
MeSH terms
Grants and funding
- R03 DA026099/DA/NIDA NIH HHS/United States
- U24 MH100929/MH/NIMH NIH HHS/United States
- U01 MH083500/MH/NIMH NIH HHS/United States
- AI07126/AI/NIAID NIH HHS/United States
- CA16042/CA/NCI NIH HHS/United States
- R24 NS038841/NS/NINDS NIH HHS/United States
- P30 CA016042/CA/NCI NIH HHS/United States
- N01 MH032002/MH/NIMH NIH HHS/United States
- DA026099/DA/NIDA NIH HHS/United States
- DA07683/DA/NIDA NIH HHS/United States
- DA10442/DA/NIDA NIH HHS/United States
- MH083500/MH/NIMH NIH HHS/United States
- NS038841/NS/NINDS NIH HHS/United States
- T32 AI007126/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
