

Identification of losses to follow-up in a community-based antiretroviral therapy clinic in South Africa using a computerized pharmacy tracking system
- PMID: 21078148
- PMCID: PMC3000400
- DOI: 10.1186/1471-2334-10-329
Identification of losses to follow-up in a community-based antiretroviral therapy clinic in South Africa using a computerized pharmacy tracking system
Abstract
Background: High rates of loss to follow-up (LTFU) are undermining rapidly expanding antiretroviral treatment (ART) services in sub-Saharan Africa. The intelligent dispensing of ART (iDART) is an open-source electronic pharmacy system that provides an efficient means of generating lists of patients who have failed to pick-up medication. We determined the duration of pharmacy delay that optimally identified true LTFU.
Methods: We conducted a retrospective cross-sectional study of a community-based ART cohort in Cape Town, South Africa. We used iDART to identify groups of patients known to be still enrolled in the cohort on the 1st of April 2008 that had failed to pick-up medication for periods of ≥ 6, ≥ 12, ≥ 18 and ≥ 24 weeks. We defined true LTFU as confirmed failure to pick up medication for 3 months since last attendance. We then assessed short-term and long-term outcomes using a prospectively maintained database and patient records.
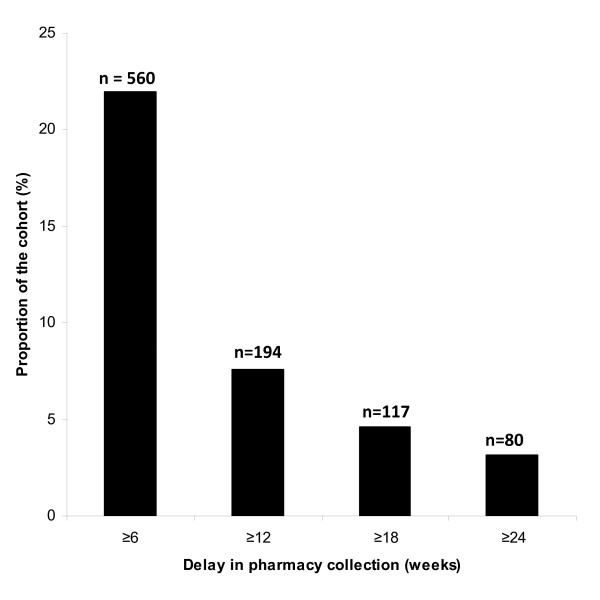
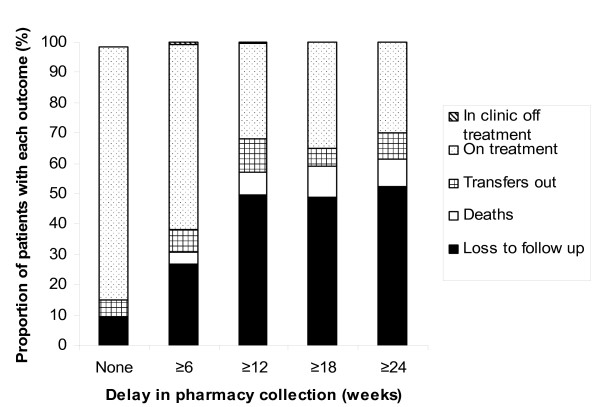
Results: On the date of the survey, 2548 patients were registered as receiving ART but of these 85 patients (3.3%) were found to be true LTFU. The numbers of individuals (proportion of the cohort) identified by iDART as having failed to collect medication for periods of ≥ 6, ≥ 12, ≥ 18 and ≥ 24 weeks were 560 (22%), 194 (8%), 117 (5%) and 80 (3%), respectively. The sensitivities of these pharmacy delays for detecting true LTFU were 100%, 100%, 62.4% and 47.1%, respectively. The corresponding specificities were 80.7%, 95.6%, 97.4% and 98.4%. Thus, the optimal delay was ≥ 12 weeks since last attendance at this clinic (equivalent to 8 weeks since medication ran out). Pharmacy delays were also found to be significantly associated with LTFU and death one year later.
Conclusions: The iDART electronic pharmacy system can be used to detect patients potentially LTFU and who require recall. Using a short a cut-off period was too non-specific for LTFU and would require the tracing of very large numbers of patients. Conversely prolonged delays were too insensitive. Of the periods assessed, a ≥ 12 weeks delay appeared optimal. This system requires prospective evaluation to further refine its utility.
Figures
References
-
- World Health Organisation. Towards universal access. scaling up priority HIV/AIDS interventions in the health sector. Progress Report 2009. World Health Organisation, Geneva. 2010. http://www.who.int/hiv/pub/tuapr_2009_en.pdf
-
- Wood R, Kaplan R, Bekker LG, Brown S, Rivett U. The utility of pharmacy dispensing data for ART programme evaluation and early identification of patients lost to follow-up. S Afr J of HIV Med. 2008. pp. 44–48.
-
- Bekker LG, Myer L, Orrell C, Lawn S, Wood R. Rapid scale-up of a community-based HIV treatment service: programme performance over 3 conecutive years in Gugulethu, South Africa. S Afr Med J. 2006;96:315–320. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
