

Automated external defibrillators and survival after in-hospital cardiac arrest
- PMID: 21078809
- PMCID: PMC3587791
- DOI: 10.1001/jama.2010.1576
Automated external defibrillators and survival after in-hospital cardiac arrest
Abstract
Context: Automated external defibrillators (AEDs) improve survival from out-of-hospital cardiac arrests, but data on their effectiveness in hospitalized patients are limited.
Objective: To evaluate the association between AED use and survival for in-hospital cardiac arrest.
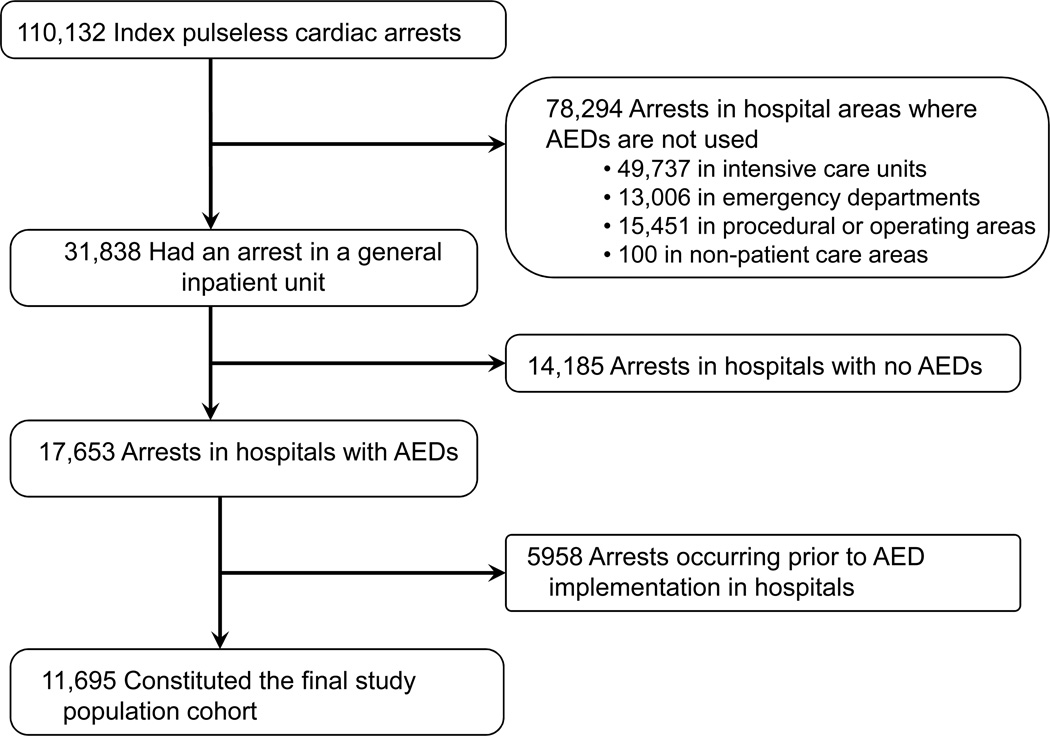
Design, setting, and patients: Cohort study of 11,695 hospitalized patients with cardiac arrests between January 1, 2000, and August 26, 2008, at 204 US hospitals following the introduction of AEDs on general hospital wards.
Main outcome measure: Survival to hospital discharge by AED use, using multivariable hierarchical regression analyses to adjust for patient factors and hospital site.
Results: Of 11,695 patients, 9616 (82.2%) had nonshockable rhythms (asystole and pulseless electrical activity) and 2079 (17.8%) had shockable rhythms (ventricular fibrillation and pulseless ventricular tachycardia). AEDs were used in 4515 patients (38.6%). Overall, 2117 patients (18.1%) survived to hospital discharge. Within the entire study population, AED use was associated with a lower rate of survival after in-hospital cardiac arrest compared with no AED use (16.3% vs 19.3%; adjusted rate ratio [RR], 0.85; 95% confidence interval [CI], 0.78-0.92; P < .001). Among cardiac arrests due to nonshockable rhythms, AED use was associated with lower survival (10.4% vs 15.4%; adjusted RR, 0.74; 95% CI, 0.65-0.83; P < .001). In contrast, for cardiac arrests due to shockable rhythms, AED use was not associated with survival (38.4% vs 39.8%; adjusted RR, 1.00; 95% CI, 0.88-1.13; P = .99). These patterns were consistently observed in both monitored and nonmonitored hospital units where AEDs were used, after matching patients to the individual units in each hospital where the cardiac arrest occurred, and with a propensity score analysis.
Conclusion: Among hospitalized patients with cardiac arrest, use of AEDs was not associated with improved survival.
Conflict of interest statement
None of the authors report any potential conflicts of interest or disclosures.
Figures
Comment in
-
Automated external defibrillators and the law of unintended consequences.JAMA. 2010 Nov 17;304(19):2178-9. doi: 10.1001/jama.2010.1674. Epub 2010 Nov 15. JAMA. 2010. PMID: 21078808 No abstract available.
-
Automated external defibrillator use for in-hospital cardiac arrest is not associated with improved survival.Evid Based Med. 2011 Jun;16(3):95-6. doi: 10.1136/ebm1195. Epub 2011 Mar 8. Evid Based Med. 2011. PMID: 21386118 No abstract available.
-
In-hospital use of automated external defibrillators does not improve survival.Aust Crit Care. 2011 Aug;24(3):210-2. doi: 10.1016/j.aucc.2011.05.003. Aust Crit Care. 2011. PMID: 21820629
References
-
- Saxon LA. Survival after tachyarrhythmic arrest--what are we waiting for? N Engl J Med. 2008;358(1):77–79. - PubMed
-
- 2005 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 5: Electrical Therapies. Circulation. 2005;112(24 Suppl):IV35–IV46. - PubMed
-
- Zafari AM, Zarter SK, Heggen V, et al. A program encouraging early defibrillation results in improved in-hospital resuscitation efficacy. J Am Coll Cardiol. 2004;44(4):846–852. - PubMed
-
- Forcina MS, Farhat AY, O'Neil WW, Haines DE. Cardiac arrest survival after implementation of automated external defibrillator technology in the in-hospital setting. Crit Care Med. 2009;37(4):1229–1236. - PubMed
-
- Weaver WD, Hill D, Fahrenbruch CE, et al. Use of the automatic external defibrillator in the management of out-of-hospital cardiac arrest. N Engl J Med. 1988;319(11):661–666. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
