

Association of serial measures of cardiac troponin T using a sensitive assay with incident heart failure and cardiovascular mortality in older adults
- PMID: 21078811
- PMCID: PMC3559101
- DOI: 10.1001/jama.2010.1708
Association of serial measures of cardiac troponin T using a sensitive assay with incident heart failure and cardiovascular mortality in older adults
Abstract
Context: Older adults comprise the majority of new-onset heart failure (HF) diagnoses, but traditional risk-factor prediction models have limited accuracy in this population to identify those at highest risk for hospitalization or death.
Objectives: To determine if cardiac troponin T (cTnT) measured by a highly sensitive assay would be detectable in the majority of community-dwelling older adults, and if serial measures were associated with risk of HF hospitalization and cardiovascular death.
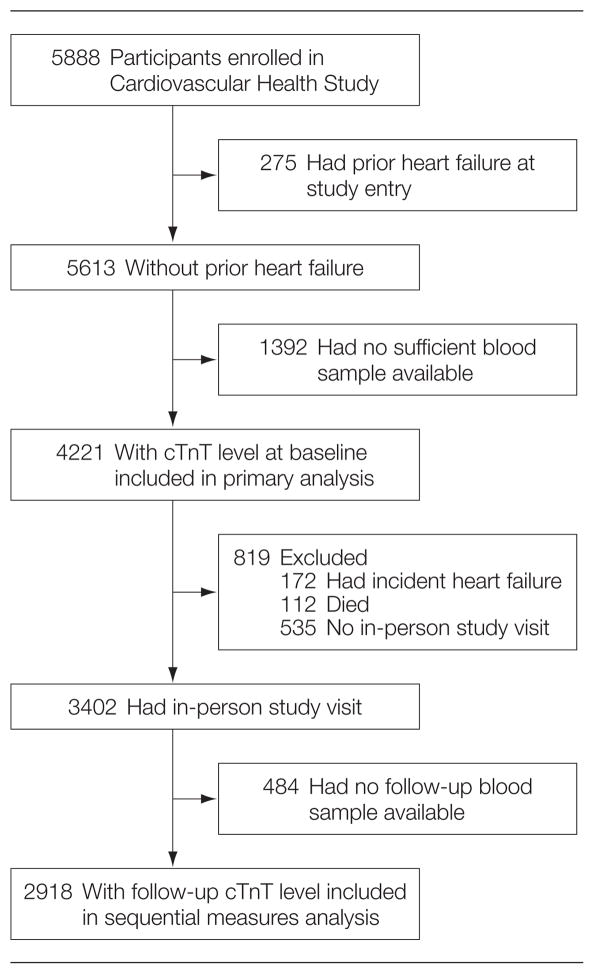
Design, setting, and participants: A longitudinal nationwide cohort study (Cardiovascular Health Study) of 4221 community-dwelling adults aged 65 years or older without prior HF who had cTnT measured using a highly sensitive assay at baseline (1989-1990) and repeated after 2 to 3 years (n = 2918).
Main outcome measures: New-onset HF and cardiovascular death were examined through June 2008 with respect to cTnT concentrations, accounting for clinical risk predictors.
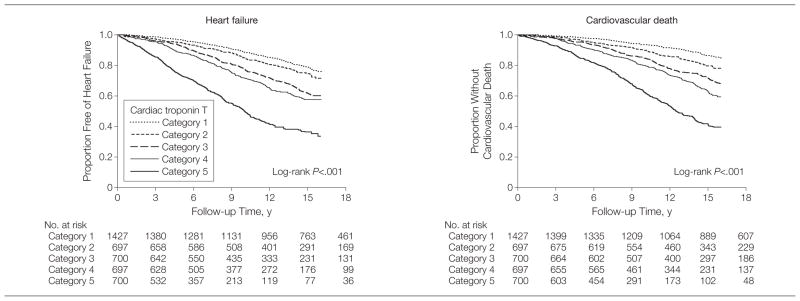
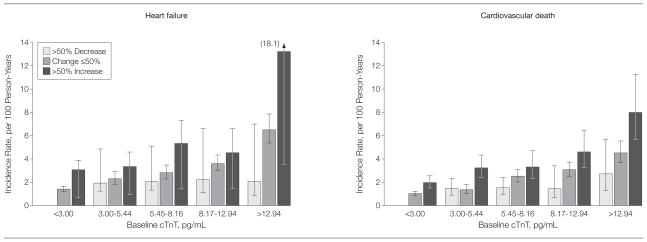
Results: Cardiac troponin T was detectable (≥3.00 pg/mL) in 2794 participants (66.2%). During a median follow-up of 11.8 years, 1279 participants experienced new-onset HF and 1103 cardiovascular deaths occurred, with a greater risk of both end points associated with higher cTnT concentrations. Among those participants with the highest cTnT concentrations (>12.94 pg/mL), there was an incidence rate per 100 person-years of 6.4 (95% confidence interval [CI], 5.8-7.2; adjusted hazard ratio [aHR], 2.48; 95% CI, 2.04-3.00) for HF and an incidence rate of 4.8 (95% CI, 4.3-5.4; aHR, 2.91; 95% CI, 2.37-3.58) for cardiovascular death compared with participants with undetectable cTnT levels (incidence rate, 1.6; 95% CI, 1.4-1.8 and 1.1; 95% CI, 0.9-1.2 for HF and cardiovascular death, respectively). Among individuals with initially detectable cTnT, a subsequent increase of more than 50% (n = 393, 22%) was associated with a greater risk for HF (aHR, 1.61; 95% CI, 1.32-1.97) and cardiovascular death (aHR, 1.65; 95% CI, 1.35-2.03) and a decrease of more than 50% (n = 247, 14%) was associated with a lower risk for HF (aHR, 0.73; 95% CI, 0.54-0.97) and cardiovascular death (aHR, 0.71; 95% CI, 0.52-0.97) compared with participants with 50% or less change. Addition of baseline cTnT measurements to clinical risk factors was associated with only modest improvement in discrimination, with change in C statistic of 0.015 for HF and 0.013 for cardiovascular death.
Conclusion: In this cohort of older adults without known HF, baseline cTnT levels and changes in cTnT levels measured with a highly sensitive assay were significantly associated with incident HF and cardiovascular death.
Figures
Comment in
-
Biomarkers: Even low cTnT levels are indicative of structural heart disease and might be useful in screening.Nat Rev Cardiol. 2011 Feb;8(2):61. doi: 10.1038/nrcardio.2010.211. Nat Rev Cardiol. 2011. PMID: 21348137 No abstract available.
-
Highly sensitive cardiac troponin T assay, cardiac disease, and mortality risk.JAMA. 2011 Mar 23;305(12):1196; author reply 1196-7. doi: 10.1001/jama.2011.345. JAMA. 2011. PMID: 21427369 No abstract available.
References
-
- Hunt SA, Abraham WT, Chin MH, et al. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure) Circulation. 2005;112(12):e154–e235. - PubMed
-
- Lloyd-Jones DM. Cardiovascular risk prediction: basic concepts, current status, and future directions. Circulation. 2010;121(15):1768–1777. - PubMed
-
- Pfisterer M, Buser P, Rickli H, et al. BNP-guided vs symptom-guided heart failure therapy: the Trial of Intensified vs Standard Medical Therapy in Elderly Patients With Congestive Heart Failure (TIME-CHF) randomized trial. JAMA. 2009;301 (4):383–392. - PubMed
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428. - PubMed
-
- D’Agostino RB, Sr, Grundy S, Sullivan LM, et al. Validation of the Framingham coronary heart disease prediction scores: results of a multiple ethnic groups investigation. JAMA. 2001;286(2):180–187. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 HL075366/HL/NHLBI NIH HHS/United States
- N01-HC-85085/HC/NHLBI NIH HHS/United States
- P30-AG-024827/AG/NIA NIH HHS/United States
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- AG-027058/AG/NIA NIH HHS/United States
- N01-HC-85082/HC/NHLBI NIH HHS/United States
- N01 HC-55222/HC/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- R01 AG020098/AG/NIA NIH HHS/United States
- N01-HC-85079/HC/NHLBI NIH HHS/United States
- N01 HC075150/HL/NHLBI NIH HHS/United States
- N01 HC035129/HC/NHLBI NIH HHS/United States
- N01-HC-85084/HC/NHLBI NIH HHS/United States
- P30 AG024827/AG/NIA NIH HHS/United States
- R01 AG-15928/AG/NIA NIH HHS/United States
- R01 AG015928/AG/NIA NIH HHS/United States
- U01 HL080295/HL/NHLBI NIH HHS/United States
- N01-HC-85081/HC/NHLBI NIH HHS/United States
- R01 HL-075366/HL/NHLBI NIH HHS/United States
- N01 HC015103/HC/NHLBI NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- N01-HC-85083/HC/NHLBI NIH HHS/United States
- N01-HC-75150/HC/NHLBI NIH HHS/United States
- N01-HC-85080/HC/NHLBI NIH HHS/United States
- R01 AG-20098/AG/NIA NIH HHS/United States
- R01 AG027058/AG/NIA NIH HHS/United States
- N01 HC045133/HC/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
