

Neurophysiological characterization of motor recovery in acute spinal cord injury
- PMID: 21079622
- PMCID: PMC3444805
- DOI: 10.1038/sc.2010.145
Neurophysiological characterization of motor recovery in acute spinal cord injury
Abstract
Study design: Prospective cohort study.
Objective: This study was designed to neurophysiologically characterize motor control recovery after spinal cord injury (SCI).
Setting: University of Louisville, Louisville, Kentucky, USA.
Material: Eleven acute SCI admissions and five non-injured subjects were recruited for this study.
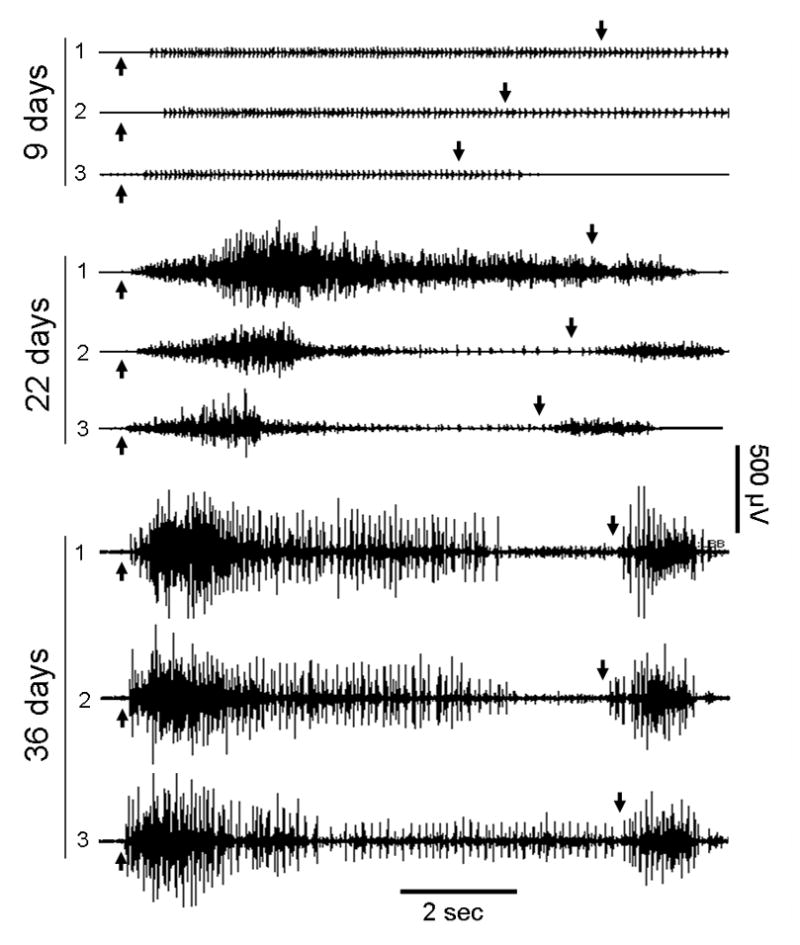
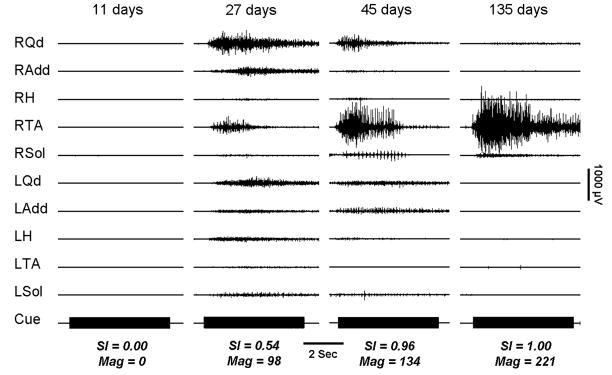
Methods: The American Spinal Injury Association Impairment Scale (AIS) was used to categorize injury level and severity at onset. Multimuscle surface electromyography (sEMG) recording protocol of reflex and volitional motor tasks was initially performed between the day of injury and 11 days post onset (6.4±3.6, mean±s.d. days). Follow-up data were recorded for up to 17 months after injury. Initial AIS distribution was as follows: 4 AIS-A; 2 AIS-C; 5 AIS-D. Multimuscle activation patterns were quantified from the sEMG amplitudes of selected muscles using a vector-based calculation that produces separate values for the magnitude and similarity of SCI test-subject patterns to those of non-injured subjects for each task.
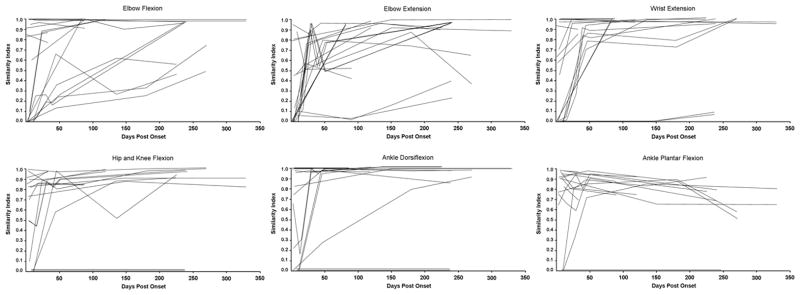
Results: In SCI subjects, overall sEMG amplitudes were lower after SCI. Prime mover muscle voluntary recruitment was slower and multimuscle patterns were disrupted by SCI. Recovery occurred in 9 of the 11 subjects, showing an increase in sEMG amplitudes, more rapid prime mover muscle recruitment rates and the progressive normalization of the multimuscle activation patterns. The rate of increase was highly individualized, differing over time by limb and proximal or distal joint within each subject and across the SCI group.
Conclusions: Recovery of voluntary motor function can be quantitatively tracked using neurophysiological methods in the domains of time and multimuscle motor unit activation.
Figures

References
-
- Yilmaz F, Sahin F, Aktug S, Kuran B, Yilmaz A. Long-Term Follow-up of Patients with Spinal Cord Injury. Neurorehabil Neural Repair. 2005;19(4):332–7. - PubMed
-
- Illis LS. The motor neuron surface and spinal shock. In: Williams Denis., editor. Modern Trends in Neurology. 0. Vol. 4. Vol. 4. Appleton-Century-Crofts; 1967. pp. 53–68. - PubMed
-
- Kakulas BA. Neuropathology: the foundation for new treatments in spinal cord injury (Sir Ludwig Guttman Lecture) Spinal Cord. 2004;42:549–563. - PubMed
-
- Marino RJ, Barros T, Biering-Sorensen F, Burns SP, Donovan WH, Graves DE, Haak M, Hudson LM, Priebe MM ASIA Neurological Standards Committee. International standards for neurological classification of spinal cord injury. J Spinal Cord Med. 2003;26 (Suppl 1):S50–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
